Public Hospital Architectural Report, Block 4-3 Building 11Design for Madness: An Architectural History of the Public Hospital in Williamsburg, Virginia
Colonial Williamsburg Foundation Library
Research Report Series - 0061
Colonial Williamsburg Foundation
Library
Williamsburg, Virginia
1990
DESIGN FOR MADNESS
AN ARCHITECTURAL HISTORY OF THE PUBLIC HOSPITAL
IN WILLIAMSBURG, VIRGINIA
Colonial Williamsburg Foundation
1986
CONTENTS
| PREFACE | |
| ACKNOWLEDGMENTS | |
| INTRODUCTION | 2 |
| CHAPTER I THE HOSPITAL IS ESTABLISHED | 5 |
| CHAPTER II THE ARCHITECT AND HIS INFLUENCE | 13 |
| CHAPTER III THE BUILDING COMMITTEE AND CONSTRUCTION | 23 |
| CHAPTER IV PLAN, FUNCTION AND USE | 34 |
| CHAPTER V NINETEENTH-CENTURY GROWTH | 45 |
| CHAPTER VI NEW DIRECTIONS, 1838-1885 | 50 |
| CHAPTER VII COLONIAL WILLIAMSBURG AND EASTERN STATE HOSPITAL, 1928-1969 | 63 |
| CHAPTER VIII RECONSTRUCTION | 70 |
| APPENDIX A | 98 |
| APPENDIX B | 101 |
| SELECTED READINGS | 103 |
| PHOTOGRAPHIC CREDITS | 106 |
INTRODUCTION
On the eve of the American Revolution a new public building joined the ranks of others that preceded it in the colonial capital of Virginia. Despite the lack of fanfare that accompanied both the its founding and its completion, the Public Hospital for "Idiots, Lunatics and Persons of Insane Mind" was unique. This last major public building constructed in Williamsburg in the colonial period holds the distinction as the first institution in America built solely for the treatment of the mentally ill. As historical circumstance would have it, the Public Hospital's beginning straddled a social watershed with one foot in the past and another in the future. Its founding looked to the past and philanthropic notions of a ruling gentry class with its commitment to the power of science and reason to change "disordered minds." Yet once it was established, the hospital was forever wedded to the reality of its function, and hence the future, regardless of the intentions of its founders. A building, such as a hospital, can be understood to be as the result of a social need, and as such, when the needs of patients and the goals of its physicians change over time, there are corresponding changes in the building's function, its use and its form. This book examines the meaning of the Public Hospital as an 3 architectural entity. An analysis of such a meaning though must take into consideration who the building served, how it functioned and the architectural context of its design. Yet sorting out the meaning for this social/architectural interdependence is as elusive as understanding the causes of mental illness. For instance, this was not a traditional building in regard to its function yet in exterior appearance, it was rather common as the image of a public building. What did the architect, who never visited Williamsburg, have in mind when he designed such a pioneer institution? How did local buildings and local construction traditions affect it? A more intriguing question bears on the interdependence of medicine and architecture in the eighteenth and nineteenth centuries. Did architectural form affect medical treatment or vice versa? Did the Public Hospital's early beginning give it an advantage as the new profession of psychiatry developed or were the early buildings a hindrance to the new stylistic trends of hospital architecture which became so prevalent in the mid-nineteenth century? These questions and others form the principal purpose of this work.
In retrospect, it seems that the reconstruction of this building within the bounds of Colonial Williamsburg's Historic Area was inevitable. The replacement of significant buildings, especially public buildings, has been considered absolutely necessary in order to fulfill the Foundation's educational goals. The reconstruction and interpretation of the 4 Public Hospital is important for a more complete history of Williamsburg in the late colonial era. It is, without a doubt, an unlikely institution in the late eighteenth-century social fabric for which Williamsburg has heretofore been portrayed. The building is also an important example in the chronological development of Williamsburg's architecture and as an example of the work of its architect and builder. A combination of these factors justifies its reconstruction. And when major buildings are reconstructed in Colonial Williamsburg, especially so long after the bulk of the restored town has taken shape, the general public is as curious about a building's modern physical history as its historical history. A brief discussion of the building's reconstruction comprises the final purpose of this work. By reviewing just some of the research and documentation, and by discussing their translation into bricks and mortar, it is hoped that the process of reconstruction will appear less mysterious and more the product of the patience, commitment, and dedication for which Colonial Williamsburg is known.
THE HOSPITAL IS ESTABLISHED
The establishment of the Public Hospital will probably always remain somewhat of a mystery. There are, of course, readily given reasons for its existence, some of which are undeniably clear. There is no doubt that the founder of the Public Hospital, Governor Francis Fauquier, was a gentleman of great intellect and large philanthropic and humanitarian interests, a man of the Enlightenment (Fig. 1). Unfortunately, Fauquier left no evidence of what specifically led him to propose Williamsburg's new public building to the House of Burgesses in the fall of 1766. Fauquier's two oft-repeated themes seem to be born of some concern for the safety of society, and a sense of obligation for affecting a cure for insanity, as mentioned in his proposal:
It is expedient I should also recommend to your Consideration and Humanity a poor unhappy set of People who are deprived of their senses and wander about the Country, terrifying the Rest of their Fellow Creatures. A legal Confinement, and proper Provision, ought to be appointed for these miserable Objects, who cannot help themselves. Every civilized Country has an Hospital for these People, where they are confined, maintained and attended by able Physicians, to endeavour to restore to them their lost Reason.1
The burgesses responded with a resolution endorsing erection of such a hospital but no action was taken. Fauquier again proposed a hospital the following spring. At that time he
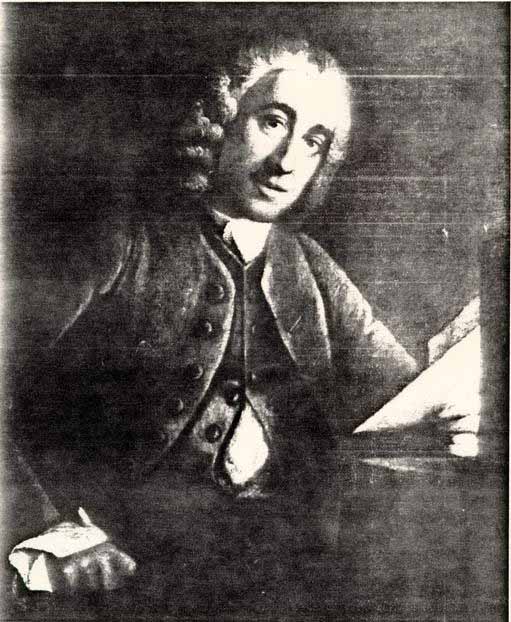 Fig. 1 Governor Francis Fauquier, Founder of the Public Hospital. (CWF #67-2033)
6
considered the hospital as "some importance to the ease and comfort of the whole community, as well as a point of charity."2 Fauquier died before making his proposal for a third time and the issue passed to his successor, Governor
Fig. 1 Governor Francis Fauquier, Founder of the Public Hospital. (CWF #67-2033)
6
considered the hospital as "some importance to the ease and comfort of the whole community, as well as a point of charity."2 Fauquier died before making his proposal for a third time and the issue passed to his successor, Governor Lord Botetourt. Perhaps helped by a Virginia Gazette editorial July 6, 1769, which referred to a murder by a lunatic that might have been prevented if a proper place of confinement existed, the House of Burgesses moved closer to enactment on November 15, 1769, when it ordered draft legislation for the hospital. Just prior to this, Botetourt asked William Byrd III to inquire of the general hospital (Fig. 2) in Philadelphia if four lunatics confined to the Public Gaol in Williamsburg might be sent there. The administrators of the Pennsylvania Hospital had set aside its cellar cells for the insane and replied favorably to the request. Both the newspaper editorial and the request by Botetourt indicate an awareness and a realization that the issue of mental illness was to some degree a social and a public matter rather than a private one. It also signified an Enlightenment belief in the power of scientific medicine. It was not until June 4, 1770, that the burgesses passed a bill to establish the Public Hospital. The enacting legislation cited both the need for restraint of those "who may be dangerous to society" and "effecting a cure" for insanity.3
Public provision for the insane in colonial America consisted of jails and, in some cases, almshouses for the indigent. With the exception of the Pennsylvania Hospital, no institutional system of treatment existed. If treatment was in
7
 Fig. 2 Pennsylvania Hospital, Philadelphia, founded in 1755. This illustration was a subscription print. The right wing was constructed in 1756; the left wing dates to 1796; and the central pavilion dates to 1804. (Historical Society of Pennsylvania)
7
evidence at all, it was a private matter for those families who had the means and the desire. Why establish such an institution in Williamsburg? After all, Williamsburg was not a bustling urban center with a disproportionately large number of the mentally ill. Virginia as a whole, in fact, had a large, yet dispersed population exceeding that of Pennsylvania, Maryland and Massachusetts, but except for the brief legislative season, when the population increased, Williamsburg remained small with a permanent population in 1770 of about 1500 people. In the first few years afterthe hospital's completion, no more than half of its twenty-four single cells were occupied. In contrast, the Pennsylvania Hospital reported a rather large number of mentally ill patients in 1770, accounting for about one third of the total patient population of 135.4 The hospital's establishment then seems to lie more with the need to control than with actual need.
Fig. 2 Pennsylvania Hospital, Philadelphia, founded in 1755. This illustration was a subscription print. The right wing was constructed in 1756; the left wing dates to 1796; and the central pavilion dates to 1804. (Historical Society of Pennsylvania)
7
evidence at all, it was a private matter for those families who had the means and the desire. Why establish such an institution in Williamsburg? After all, Williamsburg was not a bustling urban center with a disproportionately large number of the mentally ill. Virginia as a whole, in fact, had a large, yet dispersed population exceeding that of Pennsylvania, Maryland and Massachusetts, but except for the brief legislative season, when the population increased, Williamsburg remained small with a permanent population in 1770 of about 1500 people. In the first few years afterthe hospital's completion, no more than half of its twenty-four single cells were occupied. In contrast, the Pennsylvania Hospital reported a rather large number of mentally ill patients in 1770, accounting for about one third of the total patient population of 135.4 The hospital's establishment then seems to lie more with the need to control than with actual need.
Fauquier had been a director of London's Foundling Hospital and he would have been aware of specialized hospitals for the insane in England, particularly Bethlehem Hospital in London (Fig.3), where the reasoned minds of physicians grappled with those who had lost their reason. These eighteenth-century hospitals had evolved from medieval hospitals operated by benefactors and monastic nursing orders who hoped for spiritual salvation through charitable acts of mercy. The secular descendants of these hospitals, like the Foundling Hospital, were established, funded, and privately administered by mid-level
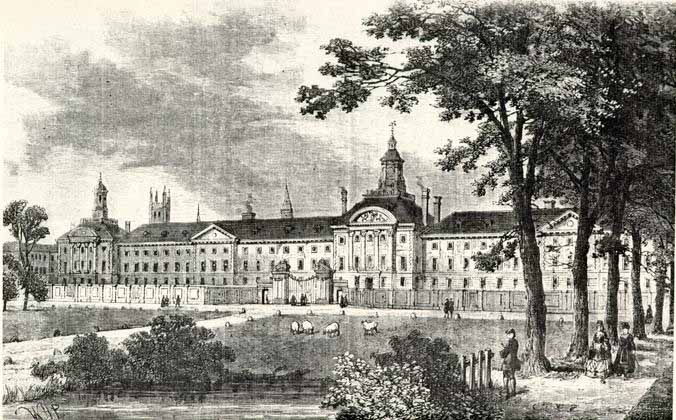 Fig. 3 Bethlehem Hospital, Moorfields, London about 1750. (CWF #84-2674)
8
gentry. Cure for the indigent and poor represented only one part of these hospital's function Moral reform was the other factor. Private subscribers, in addition to prestige, used the hospital as a device to reform and control the cost of the relief system for the poor.5 Like the voluntary hospital system in England on which it was modelled, the Public Hospital was a chance for Virginia's gentry to take control of an unruly segment of society. From June 1770 until well into the following century, the hospital would be run solely by selected trustees empowered to choose an unpaid Court of Directors consisting of a president and six other members. The first trustees had been named in the establishing legislative act: John Blair, William Nelson, Robert Carter, Peyton Randolph, Robert Carter Nicholas, John Randolph, Benjamin Waller, John Blair, Jr., George Wythe, Dudley Digges, Jr., Lewis Burwell, Thomas Nelson, Jr., Thomas Everard and John Tazewell. These men constituted political power in the colony and in the town. Seven out of ten positions in the provincial government hierarchy were represented in this group. They included all three of the colony's highest legislative officials, and as councillors four of them served in the upper house of assembly (Fig. 4). To these laymen fell the task of selecting and purchasing a site, directing construction of a building, selecting a staff, setting regulations for its operation, overseeing many administrative and financial details, and most significantly, meeting frequently to examine and decide who would be admitted or discharged.
Fig. 3 Bethlehem Hospital, Moorfields, London about 1750. (CWF #84-2674)
8
gentry. Cure for the indigent and poor represented only one part of these hospital's function Moral reform was the other factor. Private subscribers, in addition to prestige, used the hospital as a device to reform and control the cost of the relief system for the poor.5 Like the voluntary hospital system in England on which it was modelled, the Public Hospital was a chance for Virginia's gentry to take control of an unruly segment of society. From June 1770 until well into the following century, the hospital would be run solely by selected trustees empowered to choose an unpaid Court of Directors consisting of a president and six other members. The first trustees had been named in the establishing legislative act: John Blair, William Nelson, Robert Carter, Peyton Randolph, Robert Carter Nicholas, John Randolph, Benjamin Waller, John Blair, Jr., George Wythe, Dudley Digges, Jr., Lewis Burwell, Thomas Nelson, Jr., Thomas Everard and John Tazewell. These men constituted political power in the colony and in the town. Seven out of ten positions in the provincial government hierarchy were represented in this group. They included all three of the colony's highest legislative officials, and as councillors four of them served in the upper house of assembly (Fig. 4). To these laymen fell the task of selecting and purchasing a site, directing construction of a building, selecting a staff, setting regulations for its operation, overseeing many administrative and financial details, and most significantly, meeting frequently to examine and decide who would be admitted or discharged.
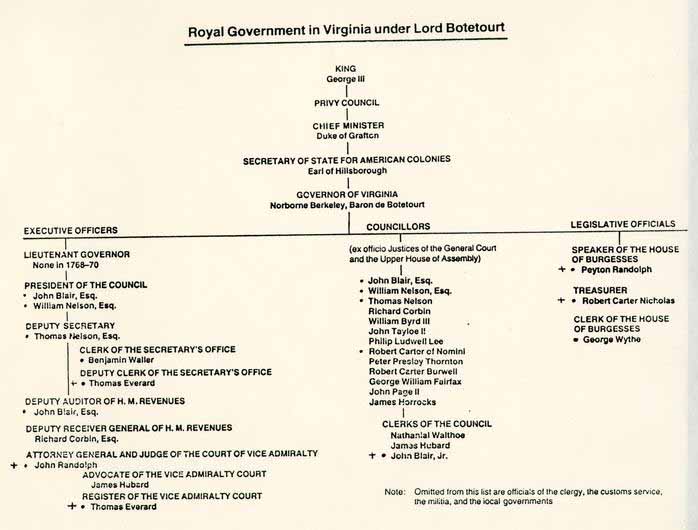 Fig. 4 Royal Government in Virginia in 1770. Public Hospital Trustees denoted by ߦ and Public Hospital Building Committee denoted by +. (Chart by John Hemphill)
Fig. 4 Royal Government in Virginia in 1770. Public Hospital Trustees denoted by ߦ and Public Hospital Building Committee denoted by +. (Chart by John Hemphill)
Yet despite the conceptual or physical prototypes, the resulting institution, although transplanted, can be seen as representative of a common theme in early American history- the imposition of a civilizing order in the American wilderness. The College of William and Mary, established in 1693, can be considered an example of intellectual order in a partially tamed wilderness. Similarly, the Public Hospital was seen as the solution to a disorder in society and for those "disordered in their senses." Establishing a "first" institution of any kind amounts to what Anthony King has characterized as a "formal acknowledgment of a change in society's arrangement for meeting a particular social need."6 The Public Hospital represented a change in the moral boundaries of the Williamsburg and Virginia communities. It was an age-old cultural, as well as medical, problem recognized in a "formal" manner by associating it with a building type that connoted both societal control, concern and public responsibility as well as an enlightenment view toward medical cure.
Although the Public Hospital was actually run by lay keepers until the 1840s, local physicians both attended the directors' meetings and treated the patients when necessary. Doctor John De Siqueyra was the first physician on call. Dr. Philip Barraud and Dr. John Minson Galt first assisted him and then succeeded him. Basically, treatment of the mentally ill was little different from the general practice of medicine in eighteenth-century America. There were special forms of 10 treatment used at the hospital, including the use of a dunking chair for plunging a patient into shockingly cold water, and the use of static electricity generated by electric machines. For the most part, traditionally-trained physicians subscribed to traditionally held medical theories based on body humors, the so-called "heroic" method.7
There were no specialists for mental illness. That field would not come into being until the mid-nineteenth century. Even the 'father of American psychiatry,' Dr. Benjamin Rush of Philadelphia, who foreshadowed the nineteenth-century Moral Management revolution in the treatment of mental illness, maintained his belief in humors in the treatment of the insane. As Norman Dain notes in his history, Disordered Minds, patients at the Public Hospital were treated well, if only by virtue of a kind keeper and staff, a small town atmosphere and an attentive group of trustees. By circumstance, then, early care and treatment at the Public Hospital was as good as comparable facilities in Philadelphia and certainly better than many of those described by John Howard in Europe.8
When the hospital opened on Tuesday, October 12, 1773, it began an uncharted course where, in its earliest period, there was a significant emphasis on cure, but the prevalent conceptions of insanity meant that the building was as much a jail as it was a hospital.9
CHAPTER I
NOTES
"… the functioning of the body and its temperment were governed by four humors, each corresponding to one of the elements that composed the cosmos. There was blood, corresponding to air and tending toward heat and moisture; phlem, corresponding to water and tending toward wet and cold; yellow or green bile (choler), corresponding to fire and tending toward heat and dryness; and black bile (whence the word "melancholy"), corresponding to earth and tending toward cold and dryness. The health of the body depended upon the maintenance of balance in these humors."
CHAPTER II
THE ARCHITECT AND HIS INFLUENCE
Stylistically, the Public Hospital fit comfortably within third-quarter of the eighteenth-century American Georgian design. It was, of course, characteristically provincial and outdated when compared to contemporary English works, such as Bootham Park Asylum in York (Fig. 5), 1772-1777, and the competition designs for the new St. Luke's Hospital in London, 1777, both for the insane and-both designed in a current neo-Palladian style. In Williamsburg, the Public Hospital slipped into the colonial capital's architectural setting like an old friend. When compared to its two late colonial contemporaries in Williamsburg, the Bruton Church tower (1769) and the Courthouse (1770), the Public Hospital held an aesthetic edge only in some of its details. Considering his ambitious architectural ideals, it is not surprising that Thomas Jefferson referred to the, college in Williamsburg and to the Public Hospital as 'rude, misshapen piles, which, but that they have roofs, would be taken for brick-kilns.'1 Jefferson thought English Georgian architecture as the 'most wretched style I ever saw' and Virginia's imitation of it as 'worse than any other part of America that I have seen.'2
Economic and social factors also played a part in the
 Fig. 5 Bootham Park Asylum, York, England. 1772-1777. (CWF #85-E11C-115O-15)
14
design process. The disputed price of imported materials for the Hospital would indicate a measure of economy in the construction of the building. Although they were concerned to a certain degree about the building's appearance, some of the trustees conscientiously valued medical over architectural treatment, such as trustee William Nelson, who stated in his will that one hundred pounds be spent for the "Relief of such poor Patients as may be sent to the said Hospital … but not to the enlargement of the Building or to any other purpose."3 If then we can consider the Public Hospital to have been organized and administered like voluntary hospitals in England, Nelson's bequest can be interpreted as a colonial extension of the English system, where ornament was "generally aschewed [at hospitals) … on the grounds that it was a misuse of charitable funds," giving eighteenth-century English voluntary hospitals an "austere and institutional appearance."4
Fig. 5 Bootham Park Asylum, York, England. 1772-1777. (CWF #85-E11C-115O-15)
14
design process. The disputed price of imported materials for the Hospital would indicate a measure of economy in the construction of the building. Although they were concerned to a certain degree about the building's appearance, some of the trustees conscientiously valued medical over architectural treatment, such as trustee William Nelson, who stated in his will that one hundred pounds be spent for the "Relief of such poor Patients as may be sent to the said Hospital … but not to the enlargement of the Building or to any other purpose."3 If then we can consider the Public Hospital to have been organized and administered like voluntary hospitals in England, Nelson's bequest can be interpreted as a colonial extension of the English system, where ornament was "generally aschewed [at hospitals) … on the grounds that it was a misuse of charitable funds," giving eighteenth-century English voluntary hospitals an "austere and institutional appearance."4
Robert Smith, architect of the Public Hospital, emigrated from Scotland to Philadelphia around 1748. When he died in 1770 at the age of 55, Smith had become one of the most accomplished carpenter-architects in America. In his lifetime, more experienced builders had gradually overtaken the amateurish gentlemen-architects for buildings both large and small. An awareness of this growing professional class of builders and the need for a specialized design, influenced the Public Hospital trustees to seek out a non-local designer.
15The connection of Smith with Williamsburg is one of the undocumented parts of the hospital's history, yet one which can be well imagined. William Byrd III of Westover is the likeliest conduit in the Williamsburg/Smith connection (Fig. 6). Byrd knew Philadelphia and corresponded with Mayor Thomas Willing of Philadelphia in 1769 regarding four lunatics in the Williamsburg Public Gaol who were eventually accommodated at the Pennsylvania Hospital.5 Byrd was the logical person to correspond with Willing, having married Willing's sister Mary in 1761.6
If Byrd did not know Robert Smith personally, Thomas Willing would have been well acquainted with Smith's work. Willing is recorded as being a trustee or subscriber to at least four buildings designed or built by Robert Smith between 1750 and 1757.7 Other Byrd-Smith connections include Dr. William Shippen and Samuel Powel, Mary Willing Byrd's uncle and brother-in-law respectively. Shippen had collaborated with Smith on the design of Nassau Hall at Princeton in 1754 and Powel had employed Smith to remodel and finish his Society Hill house, which was on Third Street across from the house of Thomas Willing and next door to the house built and occupied by William and Mary Byrd in 1761-1764. Smith's work for Powel, 1769-1773, just happened to coincide with the design of the Public Hospital.
Robert Smith and William Byrd no doubt had other mutual friends besides the Willing family, but suffice it to say, Smith's reputation would have been Byrd's assurance that he was a very capable builder-architect. The fact that
 Fig. 6 William Byrd III of Westover by Cosmo Alexandre (Virginia State Library) (CWI #56-CL-403)
16
Robert Smith's drawings, or at least his "Description" of the Hospital, were dated two months prior to the actual act establishing the institution and to the appointment of a committee to determine a design, seems clear evidence that he had been personally asked to submit a scheme. In all likelihood, Smith was chosen as the designer long before the public call for proposals.
Fig. 6 William Byrd III of Westover by Cosmo Alexandre (Virginia State Library) (CWI #56-CL-403)
16
Robert Smith's drawings, or at least his "Description" of the Hospital, were dated two months prior to the actual act establishing the institution and to the appointment of a committee to determine a design, seems clear evidence that he had been personally asked to submit a scheme. In all likelihood, Smith was chosen as the designer long before the public call for proposals.
Robert Smith was born into a Scottish family of masons and builders in Dalkeith, near Edinburgh in 1722.8 By the time of his apprentice age, there were a number.of large-scale building projects in the Edinburgh area on which Smith could have worked. One of these, the Edinburgh Royal Infirmary (Fig. 7), was designed by the famous William Adam and finished in 1748, the year Smith is believed to have emigrated.9 The Infirmary offers a tantalizing connection since it later became the design prototype for the Pennsylvania Hospital in 1754. While this Scottish hospital was not copied entirely, the Pennsylvania Hospital's individual basement cells for the insane, arranged on either side of a central passage, probably derived from the Edinburgh example (Fig. 8).10 Robert Smith probably saw the Edinburgh Royal Infirmary firsthand, but more importantly, the Pennsylvania Hospital offered a much more vivid prototype when it came to the Public Hospital.11
In comparison with his other known works, Robert Smith's designs for the Public Hospital followed a pattern established by his other public buildings. In effect, his work
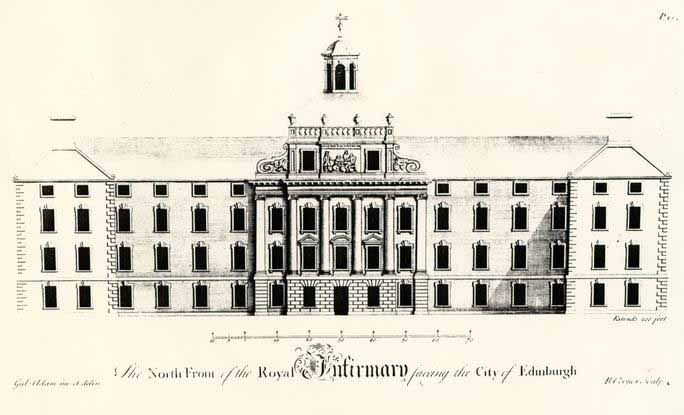 Fig. 7 Royal Infirmary, Edinburgh by William Adam, 1738-1748. From Adam's Vitruvius Scoticus. (CWF #84-2129)
Fig. 7 Royal Infirmary, Edinburgh by William Adam, 1738-1748. From Adam's Vitruvius Scoticus. (CWF #84-2129)
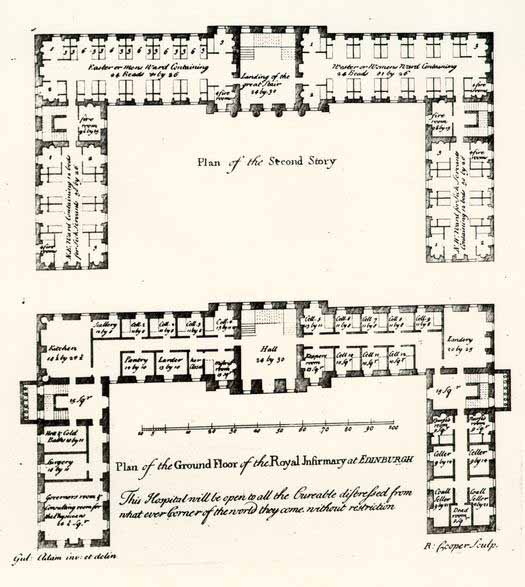 Fig. 8 Edinburgh Infirmary, ground and fourth floor plans. (William Adam, Vitruvius Scoticus) (CWF #84-2130)
17
fell into consistent types. For example, the five churches he designed and built in the decade 1757-1767 all exhibit a standard overall form and many of the same details (Fig. 9).12 This pattern is no less true of his institutional works, in the context of which the Public Hospital must be analyzed. Yet with the Public Hospital, Smith chose to continue using a very common Georgian exterior form rather than following specific and obvious hospital prototypes.
Fig. 8 Edinburgh Infirmary, ground and fourth floor plans. (William Adam, Vitruvius Scoticus) (CWF #84-2130)
17
fell into consistent types. For example, the five churches he designed and built in the decade 1757-1767 all exhibit a standard overall form and many of the same details (Fig. 9).12 This pattern is no less true of his institutional works, in the context of which the Public Hospital must be analyzed. Yet with the Public Hospital, Smith chose to continue using a very common Georgian exterior form rather than following specific and obvious hospital prototypes.
Smith's institutional work includes Nassau Hall (the University of New Jersey, later renamed Princeton University), New Jersey, 1753 (Fig. 10); Carpenters' Hall, Philadelphia, 1768 (Fig. 11); the Public Hospital, Williamsburg, 1770; and the Walnut Street Jail, Philadelphia, 1773 (Fig. 12). Typically, three of these large Georgian buildings, a college, a hospital and a prison, were functionally indistinguishable in exterior form. Each had a central pavilion, central pediment with a bull's eye window, hipped roof, and an octagonal cupola. In short, these were standard forms differing in size and details but basically similar. For the Public Hospital, Smith's design seemed to follow the rectangular form of eighteenth-century American college buildings, such as the rebuilt Wren Building, 1705, Hollis Hall at Harvard, 1762 and University Hall at Brown, 1770, rather than the "H" or "U" shaped plan with a high central pavilion that was more common to hospitals, such as the Pennsylvania Hospital or any of a number of hospitals in Scotland and England. American hospitals that came after Pennsylvania's, the New York Hospital,
Fig. 9 St. Peter's Church, Philadelphia, Robert Smith,1759. The cupola was later replaced by a steeple designed by William Strickland. (Historical Society of Pennsylvania)
Fig. 10 Nassau Hall (the University of New Jersey, later renamed Princeton University). Robert Smith, 1753. Smith also designed the Dean's House seen on the right, ca. 1754. (Princeton University Library)
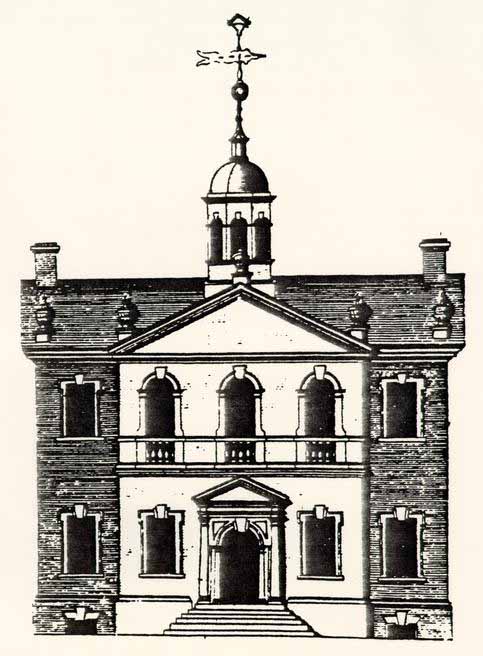 Fig. 11 Carpenters' Hall, Philadelphia, Robert Smith, 1768. (CWF #86-372)
Fig. 12 Walnut Street Jail, Philadelphia, Robert Smith, 1773. This is considered America's first penitentiary and was the structure which first drew Benjamin Henry Latrobe to Philadelphia when he was designing the Richmond Penitentiary.
18
1773-1776 (Fig. 13), and the Maryland Hospital, 1797 (Fig. 14),
both follow the Pennsylvania Hospital example. For inexplicable reasons, Smith's design for the Public Hospital did not conform in exterior appearance to obvious prototypes.13
Fig. 11 Carpenters' Hall, Philadelphia, Robert Smith, 1768. (CWF #86-372)
Fig. 12 Walnut Street Jail, Philadelphia, Robert Smith, 1773. This is considered America's first penitentiary and was the structure which first drew Benjamin Henry Latrobe to Philadelphia when he was designing the Richmond Penitentiary.
18
1773-1776 (Fig. 13), and the Maryland Hospital, 1797 (Fig. 14),
both follow the Pennsylvania Hospital example. For inexplicable reasons, Smith's design for the Public Hospital did not conform in exterior appearance to obvious prototypes.13
Smith's design for the Public Hospital was characteristic of his work only to a certain extent. Despite the fact that he had provided drawings and a written description, many details were locally derived. Eighteenth-century drawings were generally very schematic; details such as moldings, hardware, brick bond, etc. were left to the supervising builder. In the case of the Public Hospital, this person was Benjamin Powell. Robert Smith's "Description" closed with a statement referring to his recommendations as "hints" and that it was the plan that should be carefully studied. Powell, perhaps at the direction of the building committee, relied on many Smith details but rejected others. One of the few sketched details copied into the Directors' Minute Book is an example. In his "Description," Smith states that the "plinth or Water table … may be of Moulding Bricks."14 The wall section sketch depicts a two-part molded watertable that was a common Philadelphia detail (Fig. 15). It is believed that Powell ignored this recommendation and substituted a one-part bevelled watertable brick common to Williamsburg and Virginia. Similarly, Powell rejected Smith's recommendation to use stone for the foundation walls since stone is not common to the Tidewater region in Virginia. A survey of eighteenth-century buildings in Virginia will indicate a common
18a
 Fig. 13 The New York Hospital as it appeared in the early nineteenth century. The building was completed just in time to be occupied as a Revolutionary War barracks. It opened as a hospital in 1791. The building on the left is the 1808 Asylum for the insane. (CWF #84-TS-1836)
18b
Fig. 14 The Maryland Hospital for the Insane, Baltimore, 1787. Print by August Kollner, 1848. (Beale Museum)
18c
Fig. 13 The New York Hospital as it appeared in the early nineteenth century. The building was completed just in time to be occupied as a Revolutionary War barracks. It opened as a hospital in 1791. The building on the left is the 1808 Asylum for the insane. (CWF #84-TS-1836)
18b
Fig. 14 The Maryland Hospital for the Insane, Baltimore, 1787. Print by August Kollner, 1848. (Beale Museum)
18c
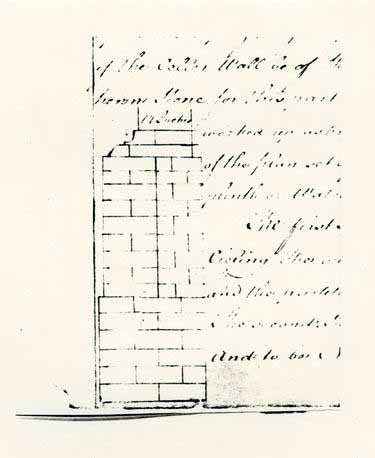 Fig. 15 Sketch of Robert Smith's proposed watertable which was copied along with his "Description" into the Hospital Directors' Minutes Book. (CWF #81-1769)
19
pool of architectural details used by local builders, just as a survey of Philadelphia, Charleston, or any other region will. Some of the Hospital's design elements can be traced to Smith's design vocabulary, seen in his other work, but due to his absence in Williamsburg, the building also reflects local materials and the building traditions of Benjamin Powell.
Fig. 15 Sketch of Robert Smith's proposed watertable which was copied along with his "Description" into the Hospital Directors' Minutes Book. (CWF #81-1769)
19
pool of architectural details used by local builders, just as a survey of Philadelphia, Charleston, or any other region will. Some of the Hospital's design elements can be traced to Smith's design vocabulary, seen in his other work, but due to his absence in Williamsburg, the building also reflects local materials and the building traditions of Benjamin Powell.
CHAPTER II
NOTES
During the construction of the Pennsylvania Hospital in 1755, Robert Smith and William Coleman were consulted about a "projection on the South side of the Ward and had given it as their Judgment that it would be no Ornament and that several Physicians were of Opinion it could not be of any Advantage to the Patients, and it appearing to be likely to cost a considerable Sum, it is now agreed to drop the said Projection." Pa. Hosp. Minutes, Volume I, 1751-1757, 29 September 1755. This reference reads as though Smith and Coleman considered the projection to be unornamental, and therefore expendable, which seems to contradict Forty's thesis, at least in this one instance.
[illegible]om its beginning, when the Pennsylvania Hospital temporarily [illegible]d a private Philadelphia house from 1751-1755, patients [illegible]ng from mental illness were admitted along with the [illegible] sick. When the new hospital opened in 1755, general [illegible]s found themselves in traditional open wards while the [illegible]were in individual cellar cells. According to a 1756 [illegible] these cells consisted of wood planks resting on a brick[illegible]ub-floor; whitewashed plaster walls with a wash board; [illegible]asings with interior shutters; and an exposed joist 22 ceiling with plaster between the joists. Upon completion of the Hospital's west wing in 1796, the insane were transferred to brick-vaulted cellar cells with brick walls and floors, all being whitewashed. Pennsylvania Hospital Minutes indicate that Robert Smith contributed L10 toward the Hospital. Charles Peterson believes that this might have been in the form of services.
It has been suggested (Peterson to McDonald) that much of the St. Peter's design was dictated to Smith through detailed specifications from the church vestry. These specifications, however, are in the form of an "agreement" or building contract, much like that made for Benjamin Powell for the Public Hospital. Contract specifications for the church could very well have followed Smith's design drawings rather than vice versa; in the case of the Public Hospital Smith's design came first, followed by the builder's contract containing specifications. Since drawings could hardly be copied into a permanent record, like the Hospital Directors' Minute Book, the drawings were most likely transferred into the written word, with many design and construction gaps filled in by the Directors.
CHAPTER III
THE BUILDING COMMITTEE AND CONSTRUCTION
After the passage of the hospital act in June 1770 the trustees moved quickly to ensure its reality. An unrecorded number of them met officially for the first Court of Directors' meeting at the Capitol on July 10, 1770. At this meeting five members were appointed as a building committee to "agree on a Plan for the HOSPITAL, and to advertise the building thereof; and also to receive Proposals for that Purpose of the several Undertakers, and to make a report of their Proceedings to the next Court."1 In less than a month the Committee, composed of Peyton Randolph, John Randolph, Robert Carter Nicholas, John Blair, Jr., and Thomas Everard, had made a decision, which was announced in the Virginia Gazette on August 2:
"The Committee appointed have, in Pursuance of the above order, agreed on a Plan for the HOSPITAL, and are ready to treat with all Undertakers, who may incline to engage in the Work. It is to be a large commodious Brick Building, and to be erected in or as near the City of Williamsburg as conveniently may be."2The plan agreed upon was that by Robert Smith. Curiously, Smith's description, which survived by virtue of its being copied into the first Court of Directors' Minutes Book, is dated April 9, 1770, a full three months before the public call for a plan. Smith's "A Description of the and Elevation of a Hospital for 24 Virginia" contained in part this general description of the building:
The Plan consists of a Hall for a Staircase, behind There is the Keepers apartment, and 12 other Rooms chiefly for the Reception of mad People. The Stairs begin near the front Door and land on /blank/ passage in the second Story. The second Story has 12 Rooms the same Dimensions as those in the first Story, and a Room over the Keepers Apartment which may serve the Managers of the Hospital to meet or may be divided which will make two other Rooms for Patients. The Hall is designed to be open as far as the landing of the Stairs the whole hight of both Storys…3
It would be interesting to know what information or instructions Smith's Williamsburg patron gave him. Had a prototype been suggested or was Smith expected to provide an appropriate design? The fact that the description was copied into the minutes without qualification indicates that the committee took the design without change. No evidence has ever placed Smith in Williamsburg, which could explain his recommendation of stone foundation walls. Being unfamiliar with the region and its building practices, Smith did not know that Tidewater Virginia is virtually without native building stone. Not surprisingly then, portions of Smith's specifications were simplified and adapted to local custom.
In September 1770 the building committee publicly announced that they would select a contractor on the 15th of the next month. In the intervening time, the committee left the "Plan and Terms" for the building with Jacob Bruce, clerk to the court, for the "Inspection of the Workmen,"4 No record of the October meeting survives but according to the building contract, 25 which was not signed until January, 1771, local builder Benjamin Powell had successfully bid the job.
Finding a builder had not occupied all of the committee's time however. Efforts had been underway during the fall to select a suitable site for the building. The legislative act had called for a site not larger than four acres and "the most healthy in situation that can be procured, and as convenient as may be to the city of Williamsburg."5 The directors reached an agreement in November and paid Thomas Walker LI12 for eight lots on the block surrounded by Francis, Henry, Ireland and Nassau Streets (Fig. 16).
The site in the southwest section of town was essentially on the boundary between the dense half-acre lots in the center of town and the open tracts that spread out from it.6 The four-acre tract bought for the hospital was part of a pattern of larger open town lots that developed on the south side of France Street, contrasting with smaller, more typical lots on the north side of the street.7 The Griffin site to the west included a house placed near the street with outbuildings and gardens fenced within its ample four-acre tract. Similarly, to the east was the four-acre Custis tract, which included 'an enclosed group of outbuildings, gardens and pasturage.8 In conformance with the adjacent property tracts, the directors ordered the entire hospital grounds enclosed by a fence almost a year before completion of the building in 1773.9 This enclosure can be seen especially well on the town maps drawn during the 26 Revolutionary War era (Fig. 17). The major departure from neighboring sites was placement of the hospital on the rear of the lot rather than near the street. This siting, for which no documented reasons exist, later became a major determining factor in the pattern of the hospital's nineteenth-century growth.
Preparations for construction began, at the earliest, in late January, 1771. Although the building committee had met in October to choose an undertaker, and a site had been purchased by December, Benjamin Powell's contract was not consummated until January 18, 1771. The hospital directors later stated that "several Months elapsed before they could engage with a Proper Person agreeable to their Wishes…."10
Benjamin Powell was a logical choice as the undertaker for the hospital construction. The Public Hospital, along with a number of projects, broke the hiatus of public building in Williamsburg since the Palace addition and the Public Records Office in the early 1750s. Powell seemingly took the lion's share, if not all of the new work in the 1760s and 1770s, due either to his experience and ability, or, perhaps to his social standing. He built an addition on the Public Gaol, the tower and steeple on Bruton Church in 1769 and he made various repairs at the Capitol and to other houses.
Being a prominent man in town, Powell held a number of public offices. He owned a number of houses and lots, including his own house near the Capitol and an 1012 acre plantation in nearby York County. Although he is most remembered as an
 Fig. 16 Detail from the Frenchman's Map, 1782, indicating a perimeter fence around the entire grounds. (CWF #N3434)
Fig. 16 Detail from the Frenchman's Map, 1782, indicating a perimeter fence around the entire grounds. (CWF #N3434)
 Fig. 17 Simcoe Map, ca. 1781, indicating a perimeter fence around the Public Hospital (number 2) with a gate [illegible] the front door. (CWF #68-2329)
27
undertaker or contractor, he is variously described as a wheelwright, carpenter and blacksmith. He directed a very successful business, engaging many laborers, craftsmen and slaves, including his own. He is also known to have trained young and orphaned apprentices in the "art and mystery of a Carpenter or Joiner."11
Fig. 17 Simcoe Map, ca. 1781, indicating a perimeter fence around the Public Hospital (number 2) with a gate [illegible] the front door. (CWF #68-2329)
27
undertaker or contractor, he is variously described as a wheelwright, carpenter and blacksmith. He directed a very successful business, engaging many laborers, craftsmen and slaves, including his own. He is also known to have trained young and orphaned apprentices in the "art and mystery of a Carpenter or Joiner."11
Powell's contract obligated him to complete the building within two years for the sum of £1,070. The contract specified that the walls were to be constructed of "hard well burnt Bricks and laid with good Mortar;" the roof to be covered in "good Cypress shingles;" the frame to be of oak or poplar; the floors "laid with Plank well seasoned one and a half inch thick and free from sap;" the cell doors to be "strong batten" and the others to be panelled. Powell was to furnish all the materials except for "Grates and such other things as are usually imported from England" and "finish and compleat the whole in a neat strong and workman like manner."12
Presumably, a number of carpenters began the task of felling oak, poplar, and pine trees in the winter of 1771. Through the spring and summer hewn and cut logs were added to the increasing inventory of finished timbers which were numbered and set aside.13 At the same time, frames for windows and doors would have been started, with the actual sash and doors following.
Meanwhile, to certain directors fell the responsibility of procuring materials "as are usually imported from England." 28 Three days following Powell's commitment to the project William Nelson wrote London merchant Robert Cary for an unspecified number of "Articles,"14 which amounted to the sizeable sum of £ 188.13..9.15 The only documented item from this order is the weathervane, recorded by virtue of a price dispute.16 Director Robert Carter was responsible for ordering the window and transom grates specified in Smith's "Description." Carter's charge was not just circumstance, he was a partner in the Baltimore Iron Works from which he ordered the grates in April 1771.17
Having coordinated the acquisition of several crucial materials by the fall of 1771, Powell could then begin construction (Fig. 18). Brick mason Samuel Spurr had been chosen by Powell earlier in the year. Spurr had previously worked for Powell at the jail and probably at the church as well.18 While the wood framing members were prepared and the grates being made, Spurr was undoubtedly making bricks and lime for the hospital, as indicated by his advertisement in the Virginia Gazette on October 3, 1771:
Both the frames for doors and windows and the grates for the same had to be on hand before Spurr began his work, even though theWilliamsburg, October 2, 1771.
THE Subscriber will give good Wages, and Accommodations, to two or three Journeymen BRICKLAYERS, for the remaining Part of the Season, to work upon the Hospital building in this City. Plenty of Bricks and Lime is ready, so that there will be no Delay. SAMUEL SPURR19
 Fig. 18 This illustration from Diderot depicts the type of activity associated with the Hospital [illegible] (CWF #85-235)
29
late starting date meant that not much would get done before cold weather halted the work.
Fig. 18 This illustration from Diderot depicts the type of activity associated with the Hospital [illegible] (CWF #85-235)
29
late starting date meant that not much would get done before cold weather halted the work.
On December 16, 1771, soon after Spurr would have started the foundations, the directors ordered that the walls be increased by one half brick from the width specified by Robert Smith. Either the builder or the mason had recommended thicker walls. Archaeology confirmed this increase of about 4" for the outer foundations walls and for the central north-south pavilion walls.20 On the average, Spurr's bricks were found to be slightly larger than the specified size.21
By February 1772, the directors had realized that there would be a building cost overrun. Just to finish the building they would have to expend thirty percent more than their appropriated £1200. In addition, they pointed out to the burgesses that other necessary expenses were apparent, including the enclosure of a "Garden and Yards for Patients to walk and take in Air in" and salaries for a keeper and matron.22 The burgesses responded with an additional charge of £800 in April of that year, the same month in which the stone steps ordered by Robert Carter Nicholas arrived from England.
Work proceeded during the spring, summer and fall of 1772, but the building was not yet finished by the scheduled completion date in January, 1773. Eight months later, however, the directors met, examined the building, found it finished "according to Agreement," and turned its operation over to James Galt, its first "Keeper of the Hospital."23 On September 16, 30 1773, an ad appeared in the Virginia Gazette informing the public of the completion and its opening date, October 12, 1773.24
CHAPTER III
NOTES
[Sept. 5, 1771]
. the Invoice of the Cross, Vane & ca amounting to 27.14..-which is received & I credit you for it in Account; but the Builder says that it is most extravagantly dear, & that he hath had one made here nearly as Good for L32 our Currency, tho' the spindle is not turned, as this is; and therefore, if no Abatement is made, I shall think they take a very unfair Advantage of Charging what they please for their goods.
[Nov. 21, 1771]
I hope you will try to get some Allowance for the Excessive Charge of the Weather Cock, which I complain'd of before or I shall think I am hardly dealt by.
[Feb. 21, 1772]
I observe the Reasons, which Mr. Millington gives for the high Price of the Vane & Ca. which I suppose I must be satisfied with tho not convinced that it was not too Dear.
"… I send 2 patterns of wood to shew the sizes of grates wanted for an hospital now building here for the reception of Lunaticks 24 of the larger size are wanted 24 of the other size are wanted, both sizes to be made of wrought iron and 48 hoocks—the directors who superintend the building expect that you signify to me the price you ask for the same, also the time you require to finish the said work—. …"These grates, which Smith must have modelled on a Philadelphia example, were shipped from Baltimore on October 2, 1771. Clement Brooke, manager of the Baltimore Iron Works listed the total weight of the grates and hooks as 2664 lbs and their cost to be £88..16..-. Robert Carter was reimbursed £90..5..6.
CHAPTER IV
PLAN, FUNCTION AND USE
The Public Hospital's exterior appearance was culturally determined by virtue of its institutional and public nature. Its familiar style associated it with a certain class of society, whose values and ideas were implicitly expressed by the establishment and purpose of the institution. Yet as we have seen, the exterior form was undifferentiated as to its function. Robert Smith designed a college and a prison which did not look all that different from the Public Hospital. If the architect used such an "ideal" exterior form, did he also design an "ideal" interior plan to facilitate the hospital's intended use and purpose? To answer this we must look to the founders, the clients, of the building, who associate it with its social role and setting; to the architect's traditional or existing prototypes, to see whether a similar need in different regions or cultures results in a similar form; and to the users of the building, who eventually indicate the success or failure of an interior spatial arrangement.
In America, the hospital system developed in a dual manner. Publicly controlled almshouse hospitals in larger cities 35 served paupers, criminals, the insane, orphans, and foundlings. In other words, all those who could not afford a physician's house call.1 Voluntary hospitals of a better nature also developed and were modelled on the subscriber-run British examples, such as the 1752 London Hospital (Fig. 19). These hospitals, for example the Pennsylvania and New York Hospitals, differed from the almshouse hospitals by having a better staff, selected patients, medical students, and a lay board of administrators. Physicians who served in these hospitals did so as a social and honorary obligation. The arrangement of space was therefore logically organized by authority, with the most public and administrative spaces being the most prominently placed.
Robert Smith arranged the Public Hospital interior in response to the four groups of people who would interact within the building. This organization meant that the public and administrative spaces were the most prominent, very much like both the British voluntary hospital prototypes and also similar to Smith's other institutional works.
Upon entering the Public Hospital through its north doors one entered an entrance and stair hall that occupied the north half of the central pavilion (Figs. 20-22). An open staircase on the east wall of this hall led to the second floor and the most prominent room in the building: the directors' meeting room. From this room the directors administered the hospital and interviewed patients for admission or discharge. There was no physician's room, indicating his relatively adjunct
 Fig. 19 The London Hospital, 1752. (CWF #84-TS-1839)
Fig. 19 The London Hospital, 1752. (CWF #84-TS-1839)
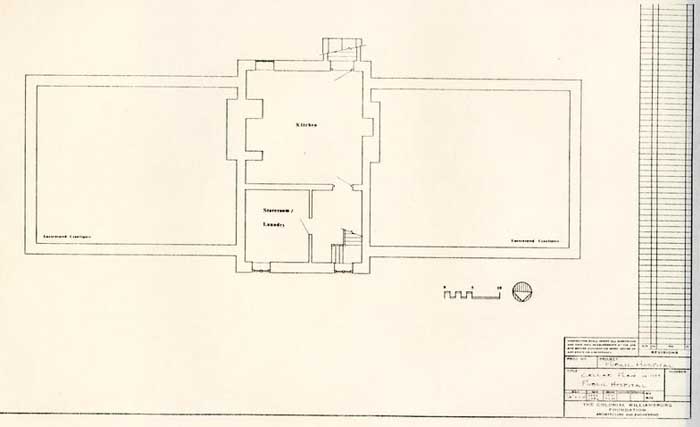 Fig. 20 Public Hospital. Reconstructed cellar plan ca. 1773. (JFW, TCM)
Fig. 20 Public Hospital. Reconstructed cellar plan ca. 1773. (JFW, TCM)
 Fig. 21 Public Hospital. Reconstructed first floor plan, ca. 1773. (JFW, TCM)
Fig. 21 Public Hospital. Reconstructed first floor plan, ca. 1773. (JFW, TCM)
 Fig. 22 Public Hospital. Reconstructed second floor plan ca. 1773. (JFW, TCM)
position at this time. Next in terms of prominence were the keeper's quarters on the first floor, separated from the entrance hall by a passage wall in the central pavilion. The keeper lived in the building and saw to the daily supervision of the patients and staff. From a central location the keeper could easily reach the cells on either floor, the hall, directors' room, the cellar, and the exterior through a south door. The staff, consisting of a matron and several attendants (both hired and slave), had use of the central pavilion cellar, which contained a kitchen, laundry and storeroom, with access through an exterior bulkhead entrance on the south or by interior stairs. The most inaccessible spaces, the cells of the patients, were reached through closed central passages in the wings of both floors. Patients were fed in their cells and went out only for exercise in the flanking exercise yards reached by east and west end doors. Physically, and in principal, this arrangement is not very different from Robert Smith's plan for Nassau Hall, where the most socially important spaces were grouped in the central pavilion with lesser functions in the wings (Fig. 23). Smith's plan for the Walnut Street Jail also had a similarly organized plan of important administrative spaces in the most publicly accessible parts of the building with the work and storage spaces and the prisoners' cells in privately controlled areas (Fig. 24). Thus, we find that a system of interior arrangement was at work, with certain basic principles applied in each case.
Fig. 22 Public Hospital. Reconstructed second floor plan ca. 1773. (JFW, TCM)
position at this time. Next in terms of prominence were the keeper's quarters on the first floor, separated from the entrance hall by a passage wall in the central pavilion. The keeper lived in the building and saw to the daily supervision of the patients and staff. From a central location the keeper could easily reach the cells on either floor, the hall, directors' room, the cellar, and the exterior through a south door. The staff, consisting of a matron and several attendants (both hired and slave), had use of the central pavilion cellar, which contained a kitchen, laundry and storeroom, with access through an exterior bulkhead entrance on the south or by interior stairs. The most inaccessible spaces, the cells of the patients, were reached through closed central passages in the wings of both floors. Patients were fed in their cells and went out only for exercise in the flanking exercise yards reached by east and west end doors. Physically, and in principal, this arrangement is not very different from Robert Smith's plan for Nassau Hall, where the most socially important spaces were grouped in the central pavilion with lesser functions in the wings (Fig. 23). Smith's plan for the Walnut Street Jail also had a similarly organized plan of important administrative spaces in the most publicly accessible parts of the building with the work and storage spaces and the prisoners' cells in privately controlled areas (Fig. 24). Thus, we find that a system of interior arrangement was at work, with certain basic principles applied in each case.
Fig. 23 Nassau Hall (College of New Jersey: Princeton). Plan by Paul Norton (?) (Princeton University Library)
Fig. 24 Walnut Street Jail, Robert Smith 1773-1777. (Library Company of Philadelphia)
37
What then were the determining factors which made this interior arrangement an "ideal" plan for the Public Hospital? The clues can be found in society's reasons for needing the institution. To reiterate, in their legislation the founders of the hospital expressed two concerns: fear and cure. Until the nineteenth century, medical treatment had little role in affecting the patients' physical environment. On the other hand, security played a great role in the purpose, function and design of the hospital. In fact, a greater alliance existed between accommodations for the insane and the criminal than with the sick. Before specialized settings were created, the insane were commonly placed in jails where the individual cell arrangement was typical, especially in large institutions (Fig. 25). In one of its roles, the Public Hospital functioned to remove a threat from society and then to separate and secure the patients from each other and from their keepers. Physical means were the rule: individual cells, barred windows, barred transoms, locked and bolted doors, high fences and walls, and one or a combination of individual leg and wrist fetters, straight jackets, or special restraining beds and chairs. Again, even if Smith had known of Scottish settings for the insane, he would have been much more familiar with the Pennsylvania Hospital. "Mechanisms" of security were typically used at the Pennsylvania Hospital, including fetters, straight jackets, heavily secured doors, high exercise yard fences, and in particular, barred windows, as documented in the hospital minutes by this 1758 reference: "It
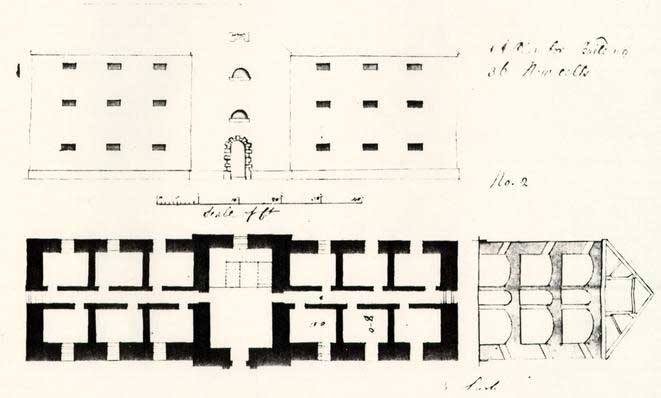 Fig. 25 Fisherton Anger County Gaol, cell block, E. Lush, 1791. The type of English county jail that might have typically held the mentally ill. Note the remarkable similarity to the Public Hospital plan. (CWF #84-TS-1835)38
appearing by the Reports that several of the Lunaticks have made their Escape owing to the iron bars of the Cells being too slender,. Tis agreed that the Monthly Committee employ the same Smith [i.e. blacksmith] who made them to make them stronger & more secure."2 When it came to designing the Public Hospital, Robert Smith's explicit description and sketches of window and transom grates expressed at least one purpose and intention of its managers.
Fig. 25 Fisherton Anger County Gaol, cell block, E. Lush, 1791. The type of English county jail that might have typically held the mentally ill. Note the remarkable similarity to the Public Hospital plan. (CWF #84-TS-1835)38
appearing by the Reports that several of the Lunaticks have made their Escape owing to the iron bars of the Cells being too slender,. Tis agreed that the Monthly Committee employ the same Smith [i.e. blacksmith] who made them to make them stronger & more secure."2 When it came to designing the Public Hospital, Robert Smith's explicit description and sketches of window and transom grates expressed at least one purpose and intention of its managers.
EARLY USE AND FUNCTION
The early use and function of the hospital can best be described as trial and adaptation. With a small patient population in its earliest years of operation, the keeper, physicians and directors slowly learned the business of a "Madhouse." Much of this business involved ordinary daily activities that might be found on a plantation with a similar number of people to feed and clothe, gardens to tend and structures to maintain. Outbuildings mentioned in 1744 are a well, a smokehouse and a house for straw (the latter being necessary for the patients' bedding). Other outbuildings joined the complex at a steady rate. Garden implements seem largely to occupy the accounts of purchased goods, along with domestic items such as candles, soap, blankets, mops, brooms, buckets, tin and 39 earthen cans and pans, wooden trays, chamberpots, etc. Clothing seemed adequate (breeches, jackets, gowns and shoes) and the extensive accounts of purchased food items indicate a surprisingly complete diet.3
Local builders, carpenters and masons applied their trades in the earliest years to make repairs to plaster walls and broken windows (planked up or filled with "dead lights"); to repair the cellar kitchen floor, chimney or hearth and to build an oven; to whitewash the interior almost annually; and frequently to construct coffins. Other-accounts reflect the specialized function of the building, which through actual use necessitated certain additions or alterations. Before the building was even finished the Directors realized that enclosed "airing" yards would be necessary and in 1772 they requested funds "inclose a Garden and Yards for Patients to walk and take the Air in."4 Although there is no mention of yards, fences or walls in either Smith's "Description" or in Powell's contract, an "airing" yard was an indispensable appendage of any facility of incarceration. European almshouses, prisons and hospitals for the insane all had their attached yards surrounded by high fences or walls. Typically, these were adjacent to the building, segregated and usually barren of amenities (Fig. 26). The fence erected by Benjamin Powell in the fall of 1773 most likely served the dual purpose of enclosing the hospital lots and providing an area for air and exercise. Due to the small number of patients during the earliest years, and to the advent of the war, it was
Fig. 26 The first Bethlehem Hospital, 1676, shown here, originally had one exercise yard at each end of the building enclosed by 14' brick walls. When the new Bethlehem Hospital was constructed in 1815 it featured numerous exercise [illegible]
40
not until about 1790 when a sufficient number of patients necessitated the addition of 80' x 30' exercise yard fences which flanked the Hospital on each end. These paled fences, which were replaced in 1799 by ten foot high brick walls, enclosed yards that until 1800 were devoid of structures or shelters, resembling the description of an English "airing" yard "where no tree nor shrub nor flower nor blade of grass grew… ;"5 The two yards segregated the male patients from the female patients. In large hospitals for the insane, such as Bethlehem Hospital, and in prisons or almshouses, men and women were further classified by degree of illness into separate yards.6
The hospital stayed in operation during the Revolutionary War, but only barely. Petitions to the governor and the House of Delegates throughout the war years consistently refer to the shortage of operating funds, supplies, and salaries for the keeper and physicians. These problems forced the hospital to close sometime around 1781, but by 1786 a new General Assembly act of incorporation had put it back in business.
Years of neglect necessitated extensive repairs after this hiatus. But more importantly, a level of full operation in the late 1780s led to alterations that indicated the interaction of patients and staff in the building. One of the obvious oversights in Robert Smith's interior plan was the reliance on one stairway to the second floor. By its placement, this one staircase served all of the user groups: the directors, the staff, and the patients. For patients to be taken from the 41 second floor out to the exercise yards, they had to walk through the entrance hall, the most public space. It was apparently decided that this created a circulation problem, and staircases were ordered built at each end of the passages in 1790, providing a more private means of circulation for both staff and patients.7
Other alterations at about this same time include the partition dividing the keeper's quarters into two rooms and the addition of isolation cells in the cellar for patients with the "raving phrensy."8 This last alteration foreshadowed the classification system that become a major aspect of the Moral Management era in the nineteenth century. In effect, there was some acknowledgement at this time that separating patients by degreeseverity of disorder would be beneficial to the patients, especially those with less severe problems.
The new state government's commitment to reopen and reestablish the Public Hospital in 1786 was a crucial one. Continuance of the institution after the war meant that it had become the first state-controlled hospital for the insane in America. Equally important, it had been given new life at a time when the townWilliamsburg needed an economic anchor. Onley Winsor, who visited Williamsburg just after the repairs in 1786, left a graphic picture of the hospital's physical relationship to the town at that time.
Here is a large handsome brick Mad House (for Lunaticks +c)--all the public buildings except the Mad House, are in a decaying situation, as most of the Private buildings, business having almost entirely left this place since the removal of the Government.942
By June 1799 the directors announced to the public that the hospital was full and would not accept new patients. With the new century the hospital steadily expanded in both its number of patients and number of buildings. The hospital was also entering the age of the American psychiatric profession, an age in thiswhich? hospital architecture and medical treatment became much more closely allied.
CHAPTER IV
NOTES
Asylum reformer Dorothea L. Dix described an exercise yard in a Pennsylvania facility in 1844:
About half the patients last August, had the liberty of the premises; others were confined in their cells or to the wards, and a few were ranging a small enclosure called the exercise yard. This miserable place was utterly comfort-less, exposed and inconvenient. The hot sun beat down upon the unconscious or half conscious patients. With bare head exposed to the direct and burning rays, they strayed around the small area, or lay extended upon the ground. Not a tree even shaded the place, and one almost felt that it was but an additional evil that they were permitted to be abroad, exposing them to the sun 44 or the tempest, the drought, the heat, or the cold, according to the season.Dorothea L. Dix, Memorial Soliciting a State Hospital for the Insane, Submitted to the Legislature of Pennsylvania, February 3, 1845. Library of Congress.
CHAPTER V
NINETEENTH-CENTURY GROWTH
By 1804 outbuildings had accumulated to the south of the hospital, giving the site a full range of subsidiary domestic structures: well, smokehouse, house for straw, privies, stable, dairy, corn crib, sheds, and a bath house.1 A small one-and-a-half story house, which came with the property just south of Ireland Street, eventually served as the matron's residence (Fig. 27). By this time, a wooden fence enclosed the entire hospital site; gardens, with their own fences, occupied part of the enclosed grounds; ten-foot-high brick walls had replaced the exercise yard fences flanking the hospital; and the exercise yards contained "covered walks" for the patients. Because the hospital had continued to run at capacity since 1799, an additional building for "the accommodation of the patients, the keeper and matron" was constructed in 1804-1805 as a detached structure slightly south and east of the main building. The new building was later referred to as the convalescent of "bettering house." An 1821 insurance policy described this building as "brick with a wooden roof, two stories high, and 32' x 18'."2
Minutes of the Board of Directors are missing for the period 1801-1822, but repair accounts do survive and indicate a wide range of maintenance work. Typifying this maintenance work are three accounts by a bricklayer, a carpenter and a blacksmith.
 Fig. 27 Dr. Philippe Pinel, one of the pioneers of moral management theories. (CWF #81-FD-4376)
46
Bricklayer James Semple's 1805 account shows that he repaired ovens, chimney backs, doors, and windows; underpinned a smokehouse, stable and necessary; built a well; laid a brick cellar floor; did plaster work; and whitewashed 27 rooms. In 1811 carpenter John Bowden replaced or installed window glass, locks, doors and door sills, floors, steps, washboards, and cellar caps. He also made coffins. Blacksmith James Hay's account from 1815 documents a wide range of work: repairing keys, locks, carts, wheelbarrows, hasps, tools, and a ducking chair. There are also many references to Hay altering or repairing leg irons and chains; typical eighteenth-and early-nineteenth century leg irons required a blacksmith to put them on and take them off.3
Fig. 27 Dr. Philippe Pinel, one of the pioneers of moral management theories. (CWF #81-FD-4376)
46
Bricklayer James Semple's 1805 account shows that he repaired ovens, chimney backs, doors, and windows; underpinned a smokehouse, stable and necessary; built a well; laid a brick cellar floor; did plaster work; and whitewashed 27 rooms. In 1811 carpenter John Bowden replaced or installed window glass, locks, doors and door sills, floors, steps, washboards, and cellar caps. He also made coffins. Blacksmith James Hay's account from 1815 documents a wide range of work: repairing keys, locks, carts, wheelbarrows, hasps, tools, and a ducking chair. There are also many references to Hay altering or repairing leg irons and chains; typical eighteenth-and early-nineteenth century leg irons required a blacksmith to put them on and take them off.3
The location of outbuildings to the south of the hospital on the four-acre site necessitated the placement of any new buildings for patients to the north or front of the original building (Fig. 28). The first of these additions was a 40' x 33' two-story brick building containing twelve cells, constructed in 1820-22 just to the northeast of the original building. This $4,000 building, which was roughly equal in both size and accommodation to one wing of the original building, was duplicated with a corresponding building to the northwest of the original building in 1824-25. These flanking buildings can be seen in a drawing believed to have been executed by keeper Dickie Galt in 1829 that shows the north elevation of the original building after the addition in 1828 of a "portico" or porch and
 Fig. 28 The Galt Cottage. (CWF #66-791)
47
the replacement of original window sash and sills (Fig. 29). The full range of cellar windows is a mystery, since archaeologists found that originally the cellar was confined to the pavilion. The dotted lines connecting the buildings represent the 10 foot high brick walls enclosing the exercise yards. If the two buildings identified on the drawing as a kitchen and laundry are switched, the kitchen plan corresponds to the detached kitchen documented by archaeology.4
Fig. 28 The Galt Cottage. (CWF #66-791)
47
the replacement of original window sash and sills (Fig. 29). The full range of cellar windows is a mystery, since archaeologists found that originally the cellar was confined to the pavilion. The dotted lines connecting the buildings represent the 10 foot high brick walls enclosing the exercise yards. If the two buildings identified on the drawing as a kitchen and laundry are switched, the kitchen plan corresponds to the detached kitchen documented by archaeology.4
Additional space was again needed in 1833, prompting an extension of the 1820 and 1824 buildings to the north. From builder Albert Chewning's contract, these 20-cell additions do not seem any more advanced in details or in the use of interior space than the buildings to which they were being added, or for that matter, the original building. In fact, hospital officials directed Chewning to copy many details from the 1820 and 1824 buildings for the new additions.
This effort to use the earlier buildings as a model, at the expense of ignoring new currents of Moral Management which had developed in England and France around the turn of the century, seems to confirm the view that Dr. Alexander D. Galt's administration of the hospital did not reflect the emerging progressive concepts practiced by some of his contemporaries.5 By all accounts, his treatment of the mentally ill, and medicine in general, was extremely conservative.6
From Pinel and Tuke in France and England respectively, there came a revolutionary theory regarding the treatment of the 48 insane that stressed non-restraint, kindness, and attention to providing an un-jail-like environment for the patients (Fig. 30). The hospital evolved in relative isolation from these new advanced theories of mental health treatment until just before Dr. John M. Galt II became superintendent in 1841.
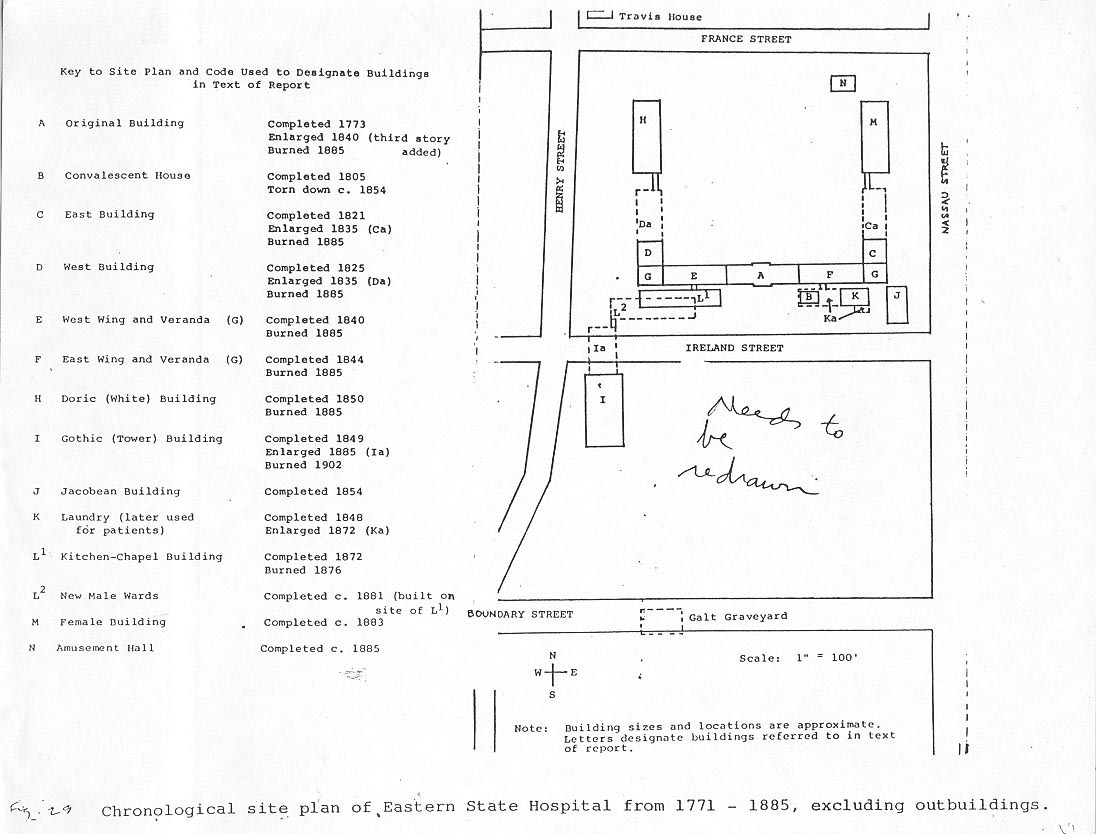 Fig. 29 Chronological site plan of Eastern State Hospital from 1771 - 1885, excluding outbuildings.
Fig. 29 Chronological site plan of Eastern State Hospital from 1771 - 1885, excluding outbuildings.
 Fig. 30 Drawing of the Public Hospital thought to be by Keeper Dickie Galt, 1829. The structures shown in plan are labelled kitchen and laundry. (CWF #81-2989)
Fig. 30 Drawing of the Public Hospital thought to be by Keeper Dickie Galt, 1829. The structures shown in plan are labelled kitchen and laundry. (CWF #81-2989)
CHAPTER V NOTES
CHAPTER VI
NEW DIRECTIONS, 1838-1885
Beginning in the 1840s, the Public Hospital left behind its isolated and idiosyncratic efforts at treatment and entered a modern "age of the asylum" era in which the superintendent was not only a physician but one trained in psychiatry. More importantly, physician-superintendents were cognizant of the tenets of Moral Management and eager to put into effect the architectural and administrative changes with which it was associated, affecting both the appearance and the function of hospitals.
A turning point came in 1838 when the directors ordered newly appointed keeper, Philip Barziza, "to make a Journey to the North for the purpose of inspecting the plans, of the principal hospitals in that quarter; taking plans of such parts as he may approve; and acquaint himself with all that may seem worthy of imitation, in the treatment of patients.1 With the director's support and a new "liberal spirit manifested by the general assembly," Barziza took charge and began instituting changes the directors hoped would 'make the success of the institution commensurate with the reasonable expectations of the public.'2 The timely appropriation for additional construction at this same time enabled the directors and Barziza to put into effect the 51 first practice of Moral Management at the hospital, changing at the last minute some of the specified details of a new building under construction to create a more domestic, less jail-like environment for the patients. They implemented these changes in a third floor addition to the original 1770 building and an adjoining three-story wing to the west where the exercise yard had been. A matching east wing was then constructed in 1842-44.
At about the same time, Dr. Stribling, a young physician who in 1836 had taken control of Western State Hospital in Staunton, Virginia (founded in 1828), made a similar inspection tour of northern asylums and also implemented architectural manifestations of Moral Management.(Fig. 31).3 The second building at Western State, constructed by 1838, features cast iron sash; a generally high level of finish in patients' rooms, including panelled doors and wire mesh transom screen; improved ventilation; and large common rooms and corridors for social interaction (Fig. 32).4 Stribling took strongly to Moral Management theories. His report to the State Assembly in 1838 probably helped inspire Eastern State Hospital directors to initiate changes.5
The American asylum grand tour was not new. In fact, it had become de rigueur for the emerging young professionals trained in the new field of psychiatry and seeking the latest in a building type which was concurrently developing as fast as their own field. Hospitals inspiring such comparative tours for architectural and medical innovation included: the Friends'
 Fig. 31 Western State Hospital; Staunton, Virginia. Constructed 1828 and shown here in 1838. The principal building is shown in its original form before the addition of porticoes. From a sketch by R. C. Lang and a drawing by A. C. smith (WSH Annual Report)
Fig. 31 Western State Hospital; Staunton, Virginia. Constructed 1828 and shown here in 1838. The principal building is shown in its original form before the addition of porticoes. From a sketch by R. C. Lang and a drawing by A. C. smith (WSH Annual Report) (CWF #86 413)
Fig. 32 An exterior cast iron sash in front of its exterior wooden equivalent. Western State Hospital, 1840s.
52
Asylum for the Insane in Pennsylvania (1817) (Fig. 33), New York's Bloomingdale Asylum (1821) (Fig. 34), the Hartford Retreat for the Insane (1824) in Connecticut (Fig. 35), the McLean Asylum for the Insane (1818) near Boston (Fig. 36), the Worcester State Lunatic Hospital (1833) in Massachusetts, and the Maryland Hospital for the Insane (1798, 1838) in Baltimore. Architect Charles Bulfinch made a tour in 1816 of hospitals in New York, Philadelphia and Baltimore before converting the Barrell House near Boston into a hospital for the insane (later named the McLean Hospital) (Fig. 37). The Pennsylvania and New York Hospital's plans are reflected in Bulfinch's double-loaded corridor of cells for the three-story wings he attached to the Barrell House. Two years later, the new superintendent/physician and an interested trustee from this new Boston asylum also made a tour of the New York and Philadelphia hospitals, this time including an inspection of the newly finished Friend's Asylum at Frankford, Pennsylvania. The Pennsylvania Hospital had in turn sent their physicians on a northern asylum inspection tour in 1848.6 It was not uncommon for architects to travel and examine new buildings, but the tours by physicians and administrators is indicative of the rate at which the two coinciding specialties were moving. Into this already changing milieu at the Eastern Lunatic Asylum, as the Public Hospital was then called, came a twenty-two-year-old doctor fresh out of medical school, who would continue in the tradition of his family's role at the Hospital. The Galts had
Fig. 33 Freind's Asylum Frankford, Pennsylvania; constructed 1817; shown here in 1835. (Historical Society of Pennsylvania)
Fig. 34 Bloomingdale Asylum, New York, constructed 1821. (New York Public Library)
Fig. 35 The Hartford Retreat; Hartford, Connecticut; constructed 1824. (Connecticut Historical Society)
Fig. 36 McLean Asylum, Boston, begun 1817, shown here in the 1840s. (Massachusetts Historical Society)
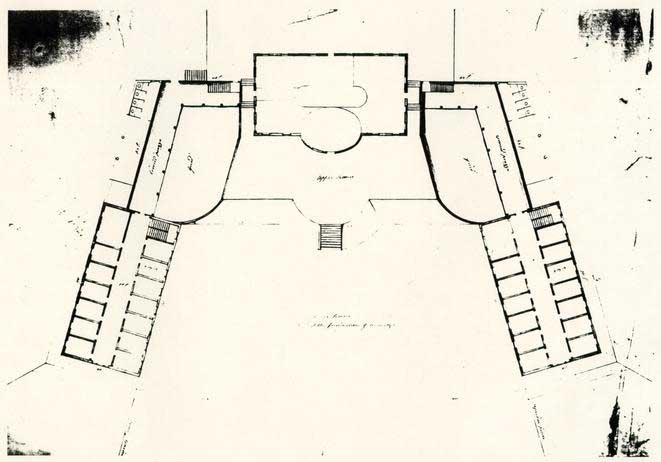 Fig. 37 Plan showing Charles Bulfinch's additions on to the Barrell Mansion, which became the McLean Asylum. (McLean Hospital) (CWF #86-414)
53
been keepers, matrons, and physicians. Now their ranks would include a professional superintendent trained in psychiatry.
Fig. 37 Plan showing Charles Bulfinch's additions on to the Barrell Mansion, which became the McLean Asylum. (McLean Hospital) (CWF #86-414)
53
been keepers, matrons, and physicians. Now their ranks would include a professional superintendent trained in psychiatry.
John Minson Galt II succeeded his father as physician at the Hospital on June 1, 1841, three months after the General Assembly's act requiring that full-time superintendents of state hospitals also be a physician (Fig. 38). This progressive step in legislation was more than equalled by the professional dedication and leadership which the young Dr. Galt brought to his field of medicine. Norman Dain's Disordered Minds and Shomer Zwelling's Quest for a Cure describe in-much more detail the personality, practice and influence of Galt. From his own 1843 tour of nine American hospitals and from the current medical works on insanity that he had ordered from Europe, Galt sought to update the appearance of his institution for both medical and aesthetic reasons. In 1843, for example, halfway through the construction of the east wing addition to the original 1770 building, Galt ordered cast iron sash, one of the hallmarks of Moral Management, for the new building and as replacements for the older window "gratings" in the rest of the buildings. To upgrade the expanding complex stylistically, Galt ordered large Greek Revival Doric porticoes in 1845 for the front of the original Public Hospital building and for its flanking advanced wings. Galt commissioned artist T. C. Millington to capture the hospital's new image on a lithograph the same year (Fig. 39).
The first major buildings constructed under the complete direction of Galt demonstrated a masterful solution that
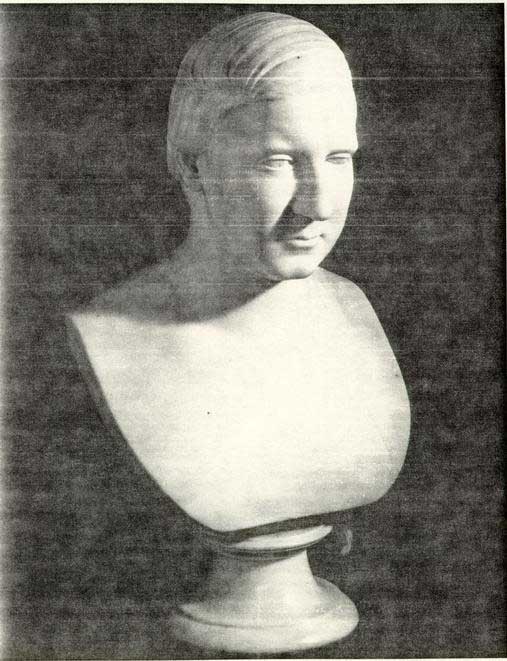 Fig. 38 John Minson Galt II. (CWF #84-PD-2207)
Fig. 38 John Minson Galt II. (CWF #84-PD-2207)
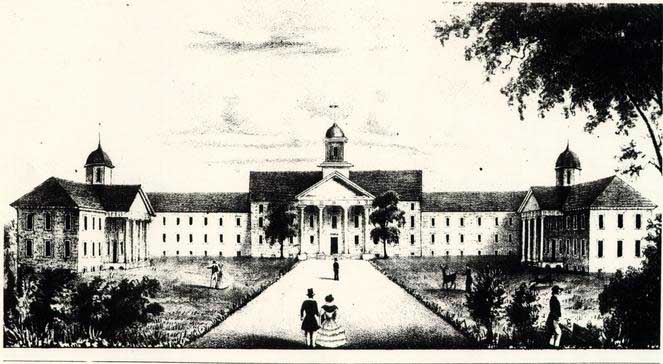 Fig. 39 Eastern State Hospital by Millington, 1845. (CWF #70-988)
54
followed advanced theories of treatment while also respecting the already established pattern of physical growth. Two buildings were begun in 1848: one for the convalescent and quiet males, and one for violent and "colored males." The separation, or "classification," of cases by severity of disorder was a common practice. Galt decided to place the quiet males' building, called the "Doric" building, to the north as a detached extension of the advanced wing; its Greek Revival classicism fit comfortably with the existing buildings that had been upgraded in the Greek Revival style (Fig. 40). The violent males, on the other hand, were placed to the south of this ordered classical complex in a "Gothic" building distinguished by two ninety foot towers (Fig. 41). This separation was necessary for reasons of treatment but the use of a very different style infers a symbolic distinction as well. This pattern was duplicated with the construction in 1854 of a "Jacobean" building (Fig. 42) to the south of the main complex for "colored patients," while the female patients were to get a classical building corresponding to the men's "Doric" building; the female building was proposed in 1855 but not constructed until 1883. From Francis Street these additions and alterations presented to the public a visual image of a well-ordered, cohesive architectural ensemble.7 Galt had thus unified the public face of the hospital by the application of Greek Revival facades to the preexisting Georgian and Federal buildings and then continued that stylistic unity in later additions.8 One obvious physical and intellectual prototype for
Fig. 39 Eastern State Hospital by Millington, 1845. (CWF #70-988)
54
followed advanced theories of treatment while also respecting the already established pattern of physical growth. Two buildings were begun in 1848: one for the convalescent and quiet males, and one for violent and "colored males." The separation, or "classification," of cases by severity of disorder was a common practice. Galt decided to place the quiet males' building, called the "Doric" building, to the north as a detached extension of the advanced wing; its Greek Revival classicism fit comfortably with the existing buildings that had been upgraded in the Greek Revival style (Fig. 40). The violent males, on the other hand, were placed to the south of this ordered classical complex in a "Gothic" building distinguished by two ninety foot towers (Fig. 41). This separation was necessary for reasons of treatment but the use of a very different style infers a symbolic distinction as well. This pattern was duplicated with the construction in 1854 of a "Jacobean" building (Fig. 42) to the south of the main complex for "colored patients," while the female patients were to get a classical building corresponding to the men's "Doric" building; the female building was proposed in 1855 but not constructed until 1883. From Francis Street these additions and alterations presented to the public a visual image of a well-ordered, cohesive architectural ensemble.7 Galt had thus unified the public face of the hospital by the application of Greek Revival facades to the preexisting Georgian and Federal buildings and then continued that stylistic unity in later additions.8 One obvious physical and intellectual prototype for
 Fig. 40 Eastern State Hospital, shown here in 1855 in a lithograph by Ramn. The building on the left in the foreground was planned at this time but not constructed until 1883. (CWF #73-1362)
Fig. 40 Eastern State Hospital, shown here in 1855 in a lithograph by Ramn. The building on the left in the foreground was planned at this time but not constructed until 1883. (CWF #73-1362)
 Fig. 41 Watercolor ca. 1860 of the "Gothic Building" by Lefevre F. Cranstone. (CWF #N4008)
Fig. 42 Views by L. A. Ramn about 1855 showing the 1820s-30s additions (with cupolas), the "Gothic Building" and the "Jacobean Building."
55
this scheme is Jefferson's design for the University of Virginia, 100 miles to the west of Williamsburg. Jefferson created his ideal academic setting, his "academical village." Galt also created an ideal setting, one of ideal rationality expressed through the reason of classical forms. Galt's renovation was not entirely an aesthetic consideration. He felt that a patient's first view of the hospital was significant, stating that "impressions of the insane mind on entering an asylum, are, sometimes of the utmost consequence; on their nature may depend the event of the case, whether the patient shall henceforth be lost in darkness of insanity, or shall regain the light of a rational mind."9 Galt wanted to create an institutional world of the sane for his patients, an environmental setting that removed patients from the physical or social conditions which had apparently caused their illness. This form of environmental treatment had its roots in Moral Management theories and became widespread among the asylum superintendents in Jacksonian America. David Rothman notes this to be a social cause-and-effect:
Fig. 41 Watercolor ca. 1860 of the "Gothic Building" by Lefevre F. Cranstone. (CWF #N4008)
Fig. 42 Views by L. A. Ramn about 1855 showing the 1820s-30s additions (with cupolas), the "Gothic Building" and the "Jacobean Building."
55
this scheme is Jefferson's design for the University of Virginia, 100 miles to the west of Williamsburg. Jefferson created his ideal academic setting, his "academical village." Galt also created an ideal setting, one of ideal rationality expressed through the reason of classical forms. Galt's renovation was not entirely an aesthetic consideration. He felt that a patient's first view of the hospital was significant, stating that "impressions of the insane mind on entering an asylum, are, sometimes of the utmost consequence; on their nature may depend the event of the case, whether the patient shall henceforth be lost in darkness of insanity, or shall regain the light of a rational mind."9 Galt wanted to create an institutional world of the sane for his patients, an environmental setting that removed patients from the physical or social conditions which had apparently caused their illness. This form of environmental treatment had its roots in Moral Management theories and became widespread among the asylum superintendents in Jacksonian America. David Rothman notes this to be a social cause-and-effect:
"The institution itself held the secret to the cure of insanity. Incarceration in a specially designed setting, not the medicines that might be administered or the surgery that might be performed there, would restore health. This strategy for treatment flowed logically and directly from the diagnosis of the causes of the disease. Medical superintendents located its roots in the exceptionally open and fluid quality of American society. The American environment had become so particularly treacherous that insanity struck its citizens with terrifying regularity.
One had only to take this dismal analysis one step further to find an antidote. Create a different kind 56 of environment, which methodically corrected the deficiencies of the community, and a cure for insanity was at hand. This, in essence, was the foundation of the asylum solution and the program that came to be known as moral treatment. The institution would arrange and administer a disciplined routine that would curb uncontrolled impulses without cruelty or unnecessary punishment. It would recreate fixity and stability to compensate for the irregularities of the society. Thus, it would rehabilitate the casualties of the system. The hospital walls would enclose a new world for the insane, designed in the reverse image of the one they had left. The asylum would also exemplify for the public the correct principles of organization. The new world of the insane would correct within its restricted domain the faults of the community and through the power or example spark a general reform movement."10
Designing a proper hospital setting along Moral Management lines was advocated and described in early nineteenth-century publications such as Andrew Duncan's Observations on the Structure of Hospitals, 1809, architect William Stark's Remarks on the Construction of Public Hospitals for the Cure of Mental Derangement, 1810, and Samuel Tuke's Description of the Retreat, published in 1816 (Figs. 43-44). To Galt, "architecture is almost as important a study to me as insanity from the intimate practical bearing which it has on the future. Therefore I should collect books in relation to it, & read on the subject at odd moments."11 Not surprisingly, Galt's library contained a number of asylum architecture books, a few examples being: William A. Browne, What Asylums Were, Are, and Ought to Be, 1837, John Conolly, The Construction and Government of Lunatic Asylums and
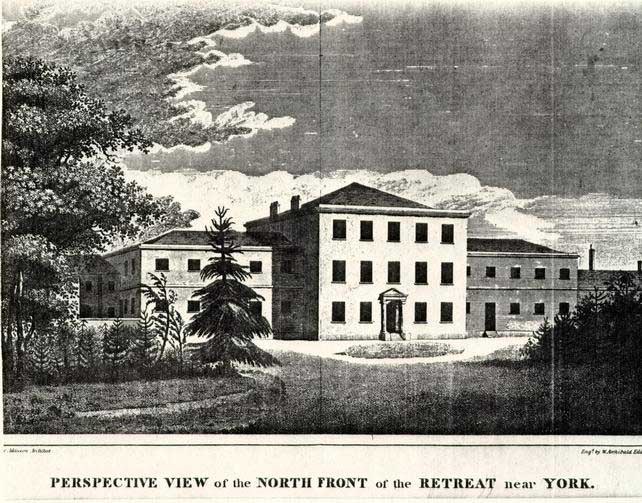 Fig. 43 The York Retreat, England. From Tuke's A Description of the Retreat. (CWF #84-1996)
Fig. 43 The York Retreat, England. From Tuke's A Description of the Retreat. (CWF #84-1996)
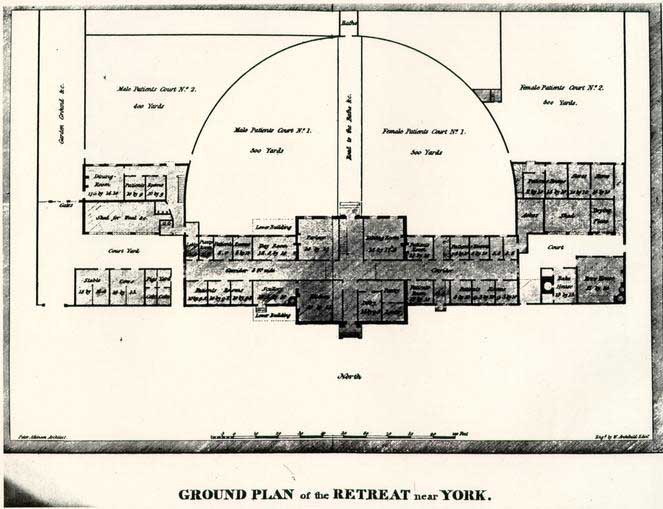 Fig. 44 York Retreat, ground plan. From Tuke's A Description of the Retreat. (CWF #84-1998)
57
Hospitals for the Insane, 1847, and Maximilian Jacobi, On the Construction and Management of Hospitals for the Insane, 1841. Galt was also certainly familiar with Thomas Kirkbride's 1847 article, "Remarks on the Construction and Arrangement of Hospitals for the Insane," which appeared in book form in 1854. Many of these treatises dealt with the construction of completely new facilities, such as Kirkbride's model asylum with its stepped-back wings (Fig. 45). Galt, of course, was constrained by the preexisting buildings and the limited size and location of the hospital property. Nevertheless, he rehabilitated the older buildings and more than doubled the hospital's acreage, although the in-town site never resembled the country setting prescribed in so many of the treatises.
Fig. 44 York Retreat, ground plan. From Tuke's A Description of the Retreat. (CWF #84-1998)
57
Hospitals for the Insane, 1847, and Maximilian Jacobi, On the Construction and Management of Hospitals for the Insane, 1841. Galt was also certainly familiar with Thomas Kirkbride's 1847 article, "Remarks on the Construction and Arrangement of Hospitals for the Insane," which appeared in book form in 1854. Many of these treatises dealt with the construction of completely new facilities, such as Kirkbride's model asylum with its stepped-back wings (Fig. 45). Galt, of course, was constrained by the preexisting buildings and the limited size and location of the hospital property. Nevertheless, he rehabilitated the older buildings and more than doubled the hospital's acreage, although the in-town site never resembled the country setting prescribed in so many of the treatises.
DECLINE, DESTRUCTION AND CONTINUANCE
John M. Galt II died in 1862 just as Civil War battles raged around Williamsburg. A series of civilian and military superintendents and a shortage of supplies brought the patient population down to 180 (the 1858 population had been 274) and the buildings to a "debilitated and deranged condition."12 Normalcy was postponed even further as the hospital suffered through a post-war period of corrupt directors (Fig. 46).
By the early 1870s the hospital seemed once again in an expansionist era (Figs. 47-48). The original 1772 building, in addition to being greatly altered by this time, had been
Fig. 45 State Hospital for the Insane, Danvers, Massachusetts. This is a typical Kirkbride plan of a model asylum. (Massachusetts Historical Society)
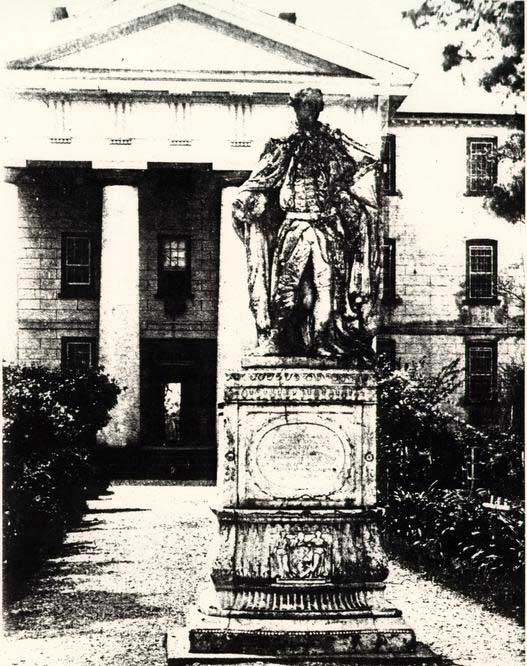 Fig. 46 North elevation of the original Hospital building, ca. 1862-64. Alterations include the addition of a third floor, scored stucco, and a Greek Revival portico and cupola. The statue of Lord Botetourt was moved to the Hospital [illegible]
Fig. 46 North elevation of the original Hospital building, ca. 1862-64. Alterations include the addition of a third floor, scored stucco, and a Greek Revival portico and cupola. The statue of Lord Botetourt was moved to the Hospital [illegible]
 Fig. 47 Drawing of Eastern State Hospital from the south by John Graham (a patient) ca. 18[illegible]-1862. (CWF #46-W-121)
Fig. 47 Drawing of Eastern State Hospital from the south by John Graham (a patient) ca. 18[illegible]-1862. (CWF #46-W-121)
 Fig. 48 Unidentified persons, presumably Dr. D. R. Brower and staff in front of the Hospital. From a photograph in the Galt Collection, Swem Library, College of William and Mary. Photograph dated 1874 on its reverse.
58
principally adapted for non-patient use, as described in this 1872 remodeling account:
Fig. 48 Unidentified persons, presumably Dr. D. R. Brower and staff in front of the Hospital. From a photograph in the Galt Collection, Swem Library, College of William and Mary. Photograph dated 1874 on its reverse.
58
principally adapted for non-patient use, as described in this 1872 remodeling account:
The first story now contains the administrative offices--a room for the Directory, a Superintendent's office, Reception room, Steward's office, Assistant Physician's room, and Dispensary; the second story, sitting rooms and bedrooms for the officers; and the third story, 19rmitories for female patients of the second class.13South of the original building a new building containing a kitchen, bakery, storeroom, chapel, amusement hall and library was completed in 1872, only to be destroyed in a fire four years later. The building which replaced it in 1881 housed only male patients, however. A new building for female patients on the east range of the extended north wings finally completed the symmetrical north range scheme depicted in the 1855 lithograph. Things seemed to be back on a smooth track: a 160 acre farm to the south had been added to the hospital property in the late 1860s; steam heating and ventilating systems had been added to the buildings in 1872; a bake house, oven, carpenter's shop, and two kitchen/storehouses were added in 1878; two infirmary wards had been created in 1882-83; an amusement hall was constructed in 1882 at the north edge of the east range near Francis Street; several buildings were remodeled or expanded in 1884-85; and electric lights were installed and operating by January 1885 (Fig. 49). Ironically, the most modern of the improvements, electricity, was held responsible for a fire on the evening of June 7, 1885. This fire destroyed the original 1773 hospital building and its 1820s-40s wings, or what the superintendent 59 described as "half the asylum." The absence of fire engines in Williamsburg, and the reliance on those sent from Richmond, resulted in the complete destruction of the building and its flanking wings.
Eastern State Hospital's physical expansion continued for the remainder of the nineteenth century and into the twentieth. After the fire, the original 1773 building's walls were dismantled to their foundations and the site covered with earth.
Before the year was up, a new administration building had been constructed just to the south of the 1773 building site (Fig. 50). The later nineteenth-century buildings were eclectic in style and reflective of the postwar custodial care era (Fig. 51).
Although new buildings replaced those which had burned, the shear problem of providing custodial care for 400-500 patients was enormous. Any architectural innovation as more likely to be the result of general building technology rather than physician input regarding treatment. In the 1890s there were repeated references by the superintendent that inappropriate and incurable patients filled the hospital. Dr. Moncure's 1893 annual report indicates that the environmental model had given way to one strictly medical, one on which he pinned his hopes:
While I believe that everything possible has been done for the welfare and the comfort of the patients committed to your care with the limited means at your disposal, I have long felt that the magnitude and great prevalence of this disease throughout all civilized countries demands that these hospitals should be placedFig. 49 South elevation of the original buildings in the year of its destruction, 1885. The pediment and cornice are believed to be reused from the 1771-1773 construction. A [illegible] lightning conduct[illegible]
Fig. 50 1885 Administration Building constructed just north of the original Hospital building site. (CWF #AL-81)
Fig. 51 The "Gothic Building" of 1848-1850 with its addition of 1883. (CWF #85-324)60 on a more thorough basis for the minute and careful study of this disease. Every modern hospital should have a trained pathologist attached to it, and whenever the medical staff deem it necessary they should have a legal right to make post-mortem examinations. These specimens should be carefully observed, their abnormal condition annotated, and the symptoms exhibited during life compared with lesions determined after death. From such study alone can progress in the treatment of insanity be expected.14


The Williamsburg institution officially signified the end of the asylum era that same year by changing its name from Eastern Lunatic Asylum to Eastern State Hospital (Fig. 52). For the first half of the twentieth century "state hospital" connoted custodial care. New therapeutic trends eventually followed custodial care: sanitariums, clinics, individual psychotherapy, milieu therapy, and networks of community-based services. Fundamentally, the emphasis has slowly switched in this century from institutions to people and human behavior as the principal agents affecting treatment. Since the 1960s the emphasis on the community as a means of treatment, and the hopes committed therein, represent another shift and perhaps another era of treatment for the mentally ill. There have been many changes to hospital architecture in the past century in accordance with various techniques and technologies. The history of a hospital demonstrates, however, that its architectural form and any changes to that form are many times associated with prevailing theories of treatment.
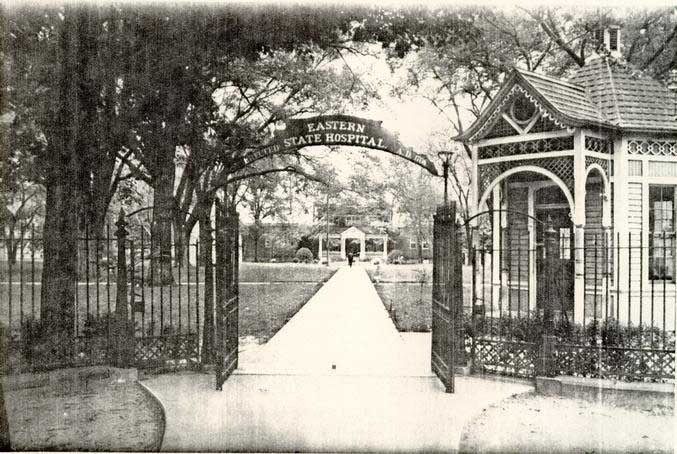 Fig. 52 Principal entrance to Eastern State Hospital showing the 1885 Administration Building and late nineteenth-century gatehouse. (CWF #AF-123)
Fig. 52 Principal entrance to Eastern State Hospital showing the 1885 Administration Building and late nineteenth-century gatehouse. (CWF #AF-123)
CHAPTER VI
NOTES
CHAPTER VII
COLONIAL WILLIAMSBURG AND EASTERN STATE HOSPITAL
1928-1969
Williamsburg's decline in the nineteenth century might have been greater had it not been for two institutions which did not require for their existence the functions of a capital. These legacies, the College of William and Mary and the Public Hospital, continued to grow in the nineteenth century and probably helped save Williamsburg from a fate similar to that of Jamestown (Fig. 53). Although it was the newer institution of the two, the Public Hospital, which eventually became known as Eastern State Hospital, actually grew much larger than the College and even as late as the mid-twentieth century its name was synonymous with that of the town. The College and the Hospital were frequently associated, often humorously:(the only difference between the two being the requirement that at the Hospital one had to at least show progress in order to leave.)1 Interestingly, it is the twentieth century association of the two that bears most heavily on the reconstruction story.
The first documented reference to reconstructing the Public Hospital as part of the restored town came at the very beginning of the restoration effort. The idea came from the Reverend William A. R. Goodwin, who through his conception of a restored town had secured the backing of John D. Rockefeller, Jr.
 Fig. 53 The scale of Eastern State Hospital, center right, clearly dominates the town in this 1928 photograph. (CWF #79-1407)
64
and elevated Williamsburg to a special small town status. Writing from the Wythe House to one of Rockefeller's organizers on February 3, 1928, Goodwin mentions that it was Eastern State Hospital Superintendent, Dr. George W. Brown, who had first attempted to find funds to "restore" the original hospital building, which had been destroyed in 1885. Dr. Brown had been discouraged by the lack of interest, lamenting that 'people of means give enumerable buildings to Colleges, but seldom any to lunatic asylums."2 Goodwin suggested asking "Mr. David" [Rockefeller] for the funds to "restore" the Hospital and at the same time acquire the colonial Galt Cottage and some land from Eastern State Hospital. Goodwin suggested that just a reconstructed facade be added to the existing 1885 administration building, which had been built just south of the original building's site. By doing this, Goodwin concluded, "we would then have included in our plan of restoration the first College building in America, the first Capitol, the first Palace, (as far as I know), the first English incorporated city in America, and the first building for the exclusive care of the insaneߪ "3 Nothing came of this initial scheme but it was the beginning of probably the longest and greatest effort by the Colonial Williamsburg Foundation to acquire an historic site in the designated Historic Area of Williamsburg.
Fig. 53 The scale of Eastern State Hospital, center right, clearly dominates the town in this 1928 photograph. (CWF #79-1407)
64
and elevated Williamsburg to a special small town status. Writing from the Wythe House to one of Rockefeller's organizers on February 3, 1928, Goodwin mentions that it was Eastern State Hospital Superintendent, Dr. George W. Brown, who had first attempted to find funds to "restore" the original hospital building, which had been destroyed in 1885. Dr. Brown had been discouraged by the lack of interest, lamenting that 'people of means give enumerable buildings to Colleges, but seldom any to lunatic asylums."2 Goodwin suggested asking "Mr. David" [Rockefeller] for the funds to "restore" the Hospital and at the same time acquire the colonial Galt Cottage and some land from Eastern State Hospital. Goodwin suggested that just a reconstructed facade be added to the existing 1885 administration building, which had been built just south of the original building's site. By doing this, Goodwin concluded, "we would then have included in our plan of restoration the first College building in America, the first Capitol, the first Palace, (as far as I know), the first English incorporated city in America, and the first building for the exclusive care of the insaneߪ "3 Nothing came of this initial scheme but it was the beginning of probably the longest and greatest effort by the Colonial Williamsburg Foundation to acquire an historic site in the designated Historic Area of Williamsburg.
By the early 1930s, Eastern State Hospital, which had helped sustain the town through its declining years, became a thorn in the side of restoration effort. This first became 65 apparent in 1933 when Eastern State announced plans to build workers' houses on land south of Francis Street and opposite King Street, an extension of the vista created for the newly reconstructed Governor's Palace. Sympathetic Hospital officials were persuaded not to build on the land but refused to sell it, citing the need for a buffer zone to the east of the complex. The following year a much more serious problem presented itself. After selecting a location for the much needed Williamsburg Lodge, Foundation officials discovered that screams of Hospital patients could clearly be heard at the proposed site. The suggested solution involved removing the noisy patients to a 500 acre farm known as Dunbar, two miles outside of town, which was owned and used by the Hospital for occupational therapy. To aid in this cause, the chairman of the State Commission on Conservation and Development was invited to Williamsburg. Spending a sleepless night because of "shrieks and yells and hideous laughter," William E. Carson gave a statement to the press which referred to the increasing realization that Colonial Williamsburg was a valuable tourist asset. "Tourists," Carson said, "are not inclined to spend the night in the vicinity of a mad house."4 With a $25,000 contribution from Colonial Williamsburg for two new buildings at Dunbar, the state legislature was persuaded by the governor to pass a bill in 1936 which called for the removal of 250-300 noisy patients from the city to the farm site. In accepting the gift, the Hospital agreed to a gradual removal of the entire in-town facilities to a 66 new modern hospital complex which, by all accounts, was clearly needed. In the meantime, the Hospital agreed not to build any major additional structures in Williamsburg.
By 1945 the Hospital had reached the capacity for housing noisy patients at the Dunbar site. Progress on the new facilities had also stalled due to financing. For the next six years occasional guests staying at the Williamsburg Lodge complained of sleepless nights brought on by "howling," which reiterated the fact that the noise problem still remained.5 One visitor wrote in 1953 that the proximity of the Hospital to the Historic Area was "truly disgraceful," and that "Here within a few blocks of the Governor's Palace showing such gracious living so long ago is modern America--a truly rude awakening to reality."6
Proposals to accelerate the removal of all hospital buildings in the 1950s failed and the 207 acres_of property eventually transferred to the College of William and Mary. Atwhich 207 acres where/what is relation of it to removal? this time, approximately one-third of the 2,200 Hospital patients had been transferred to the Dunbar site, prompting one newspaper article to state that Eastern State was suffering from schizophrenia: 'The hospital's personality is distinctly split: On the one hand, old and shabby; on the other, new and shiny. It creates a situation as crippling to the life of the institution as the disease is to ailing patients.7
Between 1959 and 1966 the College finally sold three parcels of original Hospital land totalling about 24 acres to 67 Colonial Williamsburg.8 Included with this purchase were two surviving eighteenth-early nineteenth century structures: the Galt Cottage and the Custis Kitchen. All of the other structures dated to the late nineteenth century and early twentieth century (Fig. 54). By the fall of 1969 the intrusive reality of mental illness no longer distracted visitors to the Historic Area and the former Hospital site was a tabula rasa for its anxious new owners.9
 Fig. 54 Thompson Building. By the 1960s structures like this from the "Custodial Care" era were the oldest survivors at Eastern State Hospital. (CWF #66-SMT-575)
Fig. 54 Thompson Building. By the 1960s structures like this from the "Custodial Care" era were the oldest survivors at Eastern State Hospital. (CWF #66-SMT-575)
CHAPTER VII
NOTES
Feeling that the construction of the new complex had been tied up in state financing, Colonial Williamsburg initiated a radical proposal to accelerate the removal of the old Hospital buildings in town. Colonial Williamsburg was willing to loan the state $23 million dollars at a low interest rate to complete construction of the new hospital complex. The press soon brought this controversial matter before the public in a long series of editorials and articles. The issue came to an abrupt halt when it was learned that the College of William and Mary, to whom the deed of Hospital land had been conveyed in 1945, was not willing to sell any of the 207 acres to Colonial Williamsburg, stating that the land was needed for campus expansion. This turn of events led Colonial Williamsburg to withdraw its offer and all hope was lost for a speedy completion of the new hospital complex. With legislative pressure, the College finally agreed to sell the immediate site of the original Hospital, about 11 acres, to Colonial Williamsburg. Nevertheless, negotiations broke down and any further preparation at the Dunbar site stalled for about 69 five more years.
CHAPTER VIII
RECONSTRUCTION
PLANS FOR RECONSTRUCTION
The earliest documented reference to reconstructing Eastern State Hospital's original building appeared in Reverend Goodwin's letter of 1928, cited in the previous chapter. After this date, little if nothing seems to have been discussed publicly concerning the issue due to the protracted campaign to acquire the property. The possibility of reconstruction was not forgotten though, no matter how uncertain the property acquisition might have been. On the first of January, 1950, Kenneth Chorley submitted a report to John D. Rockefeller, Jr. estimating the cost of completing the "physical restoration of Colonial Williamsburg."1 Included in the restoration plan was the "Maison des Foux," as the Public Hospital was called on the Frenchman's Map. Still, Chorley was publicly silent on any plans for reconstruction, telling the Newport News Times-Herald in 1953 that Colonial Williamsburg "at this time has no definite plans for the use of the Eastern State site, nor any plans in the making."2 The only definite statement he could make was that the corporation should acquire the property as a protection to the restored area.
71There were few tangible signs of A reconstruction plan in the 1960s other than the demolition of old hospital buildings. Significant events began to occur in the 1970s, however, and they paved the way for the reconstruction of the hospital in the following decade. Archaeological investigation of the original hospital site commenced in 1972 under the direction of Resident Archaeologist Ivor Noël Hume.3 At about the same time a comprehensive documentary research report was begun by Patricia A. Gibbs and Linda H. Rowe and conjectural floor plans and elevations were developed by Director of Architectural Research Paul Buchanan and architectural draftsman James F. Waite. Two other coinciding events took place in the mid 1970s. In 1976 Carlisle H. Humelsine secured a donation of $4 million from DeWitt Wallace for a new theater in which to show "The Story of a Patriot." The following year Humelsine committed the Foundation to reconstructing the Hospital, with a first floor devoted to-interpretive purposes and a second floor to office use.4 While these two events were not originally related, a decline in visitation dictated the postponement of the theater project in 1979 and, eventually, the application of the Wallace gift to a decorative arts museum contained within the reconstructed exterior of the Public Hospital.5
In November 1979 the project was officially announced to the public and by the following June the Public Hospital Design Review Committee began the exciting, yet arduous, task of sorting through the myriad details of reconstructing a major 72 eighteenth-century building. Architectural historian Travis C. McDonald, Jr. was hired to conduct additional research, to coordinate the design process, to supervise construction, and to chronicle the project's history. The Design Review Committee was initially composed of Roy E. Graham, Resident Architect; Edward A. Chappell, Director of Architectural Research; Donna C. Hole, Architectural Research Fellow; James F. Waite, Architectural Draftsman; and Travis C. McDonald, Jr., Architectural Coordinator. The composition of the committee changed in 1982 with the departure of Graham and Hole, who were replaced by Nicholas A. Pappas, Foundation Architect, and Beatrix T. Rumford, Vice-President Museums and the Project Director.
ARCHAEOLOGICAL INVESTIGATION
Archaeology confirmed Robert Smith's specifications for the building regarding its size and shape. The original building yielded no great architectural surprises other than the presence of a cellar beneath the central pavilion alone and crawl spaces beneath the wings (Fig. 55).6 The building measured 100'-4" by 32'-5" below the watertable, dimensions which differed only slightly from Robert Smith's written specifications.The archaeologically determined dimensions were used for the reconstruction in various ways. While the exact orientation of the building did not parallel the present streets, it appeared
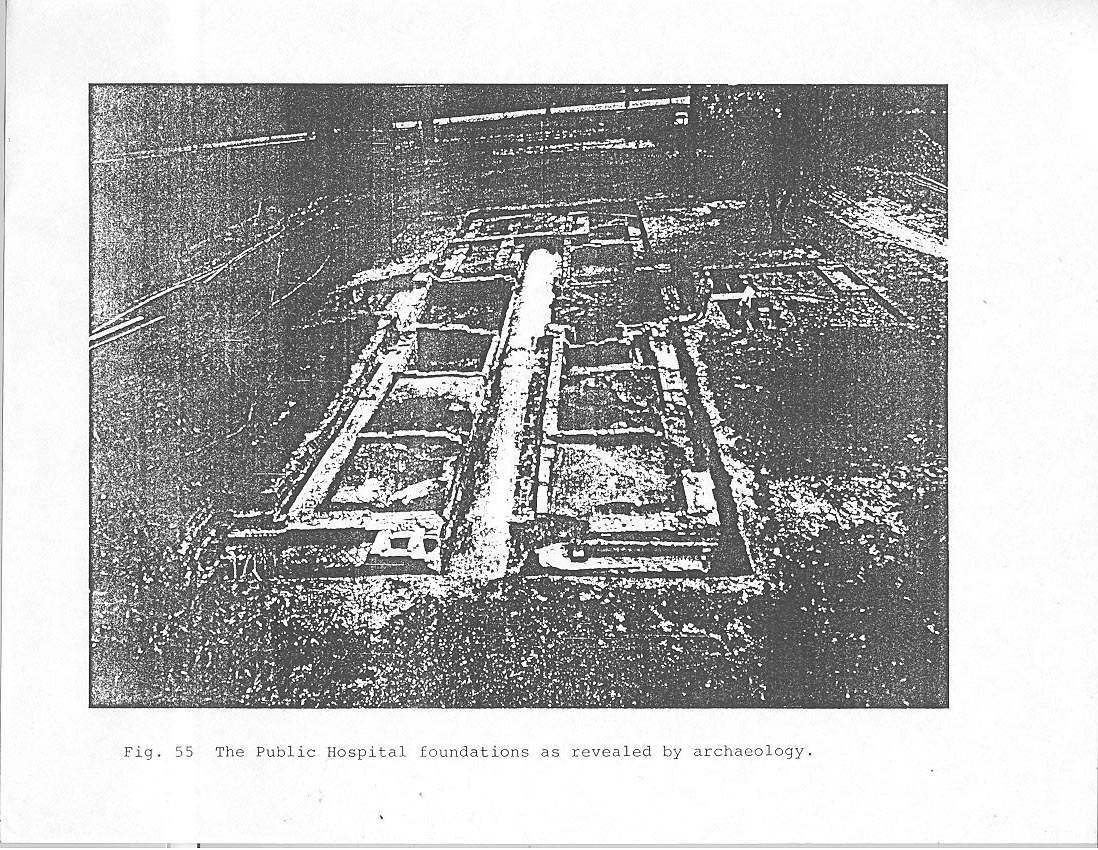 Fig. 55 The Public Hospital foundations as revealed by archaeology.
73
almost exactly in line with true north. This skewed siting was adopted for the reconstruction. Archaeology also confirmed the wall thickness and the general plan of the original building designed by Smith. It was confirmed that the walls had indeed been increased in thickness by one half brick according to the directors' instructions in 1771 and that three additional cells were added to the cellar in 1799 for patients with the "raving phrenzy." The principal room in the cellar, measuring 13' x 21'-2", showed evidence of use as a kitchen. This room was separated from the staircase and a small north cellar room by an east-west partition wall. The bulkhead entrance to the cellar was located on the south side of the pavilion. The foundation dimensions and the average brick size proved invaluable for the reconstruction design, facilitating the calculation of known horizontal and vertical dimensions by which the two historic photographs could be scaled and exterior elevations determined.
Fig. 55 The Public Hospital foundations as revealed by archaeology.
73
almost exactly in line with true north. This skewed siting was adopted for the reconstruction. Archaeology also confirmed the wall thickness and the general plan of the original building designed by Smith. It was confirmed that the walls had indeed been increased in thickness by one half brick according to the directors' instructions in 1771 and that three additional cells were added to the cellar in 1799 for patients with the "raving phrenzy." The principal room in the cellar, measuring 13' x 21'-2", showed evidence of use as a kitchen. This room was separated from the staircase and a small north cellar room by an east-west partition wall. The bulkhead entrance to the cellar was located on the south side of the pavilion. The foundation dimensions and the average brick size proved invaluable for the reconstruction design, facilitating the calculation of known horizontal and vertical dimensions by which the two historic photographs could be scaled and exterior elevations determined.
In addition to significant architectural features, the original 1773 building primarily yielded valuable artifactual information about its late nineteenth-century use. The most surprising find, unrelated to the hospital, were the remains of two seventeenth-century house sites, one of which was believed to have been Governor Francis Nicholson's residence. Based on this archaeological work, a conjectural picture of the original hospital building began to emerge.
When plans for the Wallace Gallery were formalized in 1979, additional archaeological excavations were scheduled in 74 order to record the exercise yard areas flanking the original hospital building and all of the site to the south where the proposed gallery would be located. The most significant early structures found in these areas were the 1805 Convalescent House, a late eighteenth-early nineteenth century kitchen, an 1825 kitchen complex, and a small outbuilding.
RECONSTRUCTION METHODOLOGY
Reconstructing the exterior of the Public Hospital to its earliest appearance provided the philosophical basis for both research and design (Fig. 56). The research methodology developed for the project required the study of individual architectural elements such as cellar vents, windows, doors, locks, moldings, nail patterns, joist spacing, etc. Documentation was gathered for each element, and studied by a design review committee for historical credibility and practicality. The appropriate feature was then added to the working drawings in a sequence determined by the actual schedule of construction. In most cases the basic architectural element was known, through either documentary sources or as part of conventional construction practices, but its details generally required further research. The philosophy governing the committee's decisions revolved around securely documented information. The principal sources, Robert Smith's
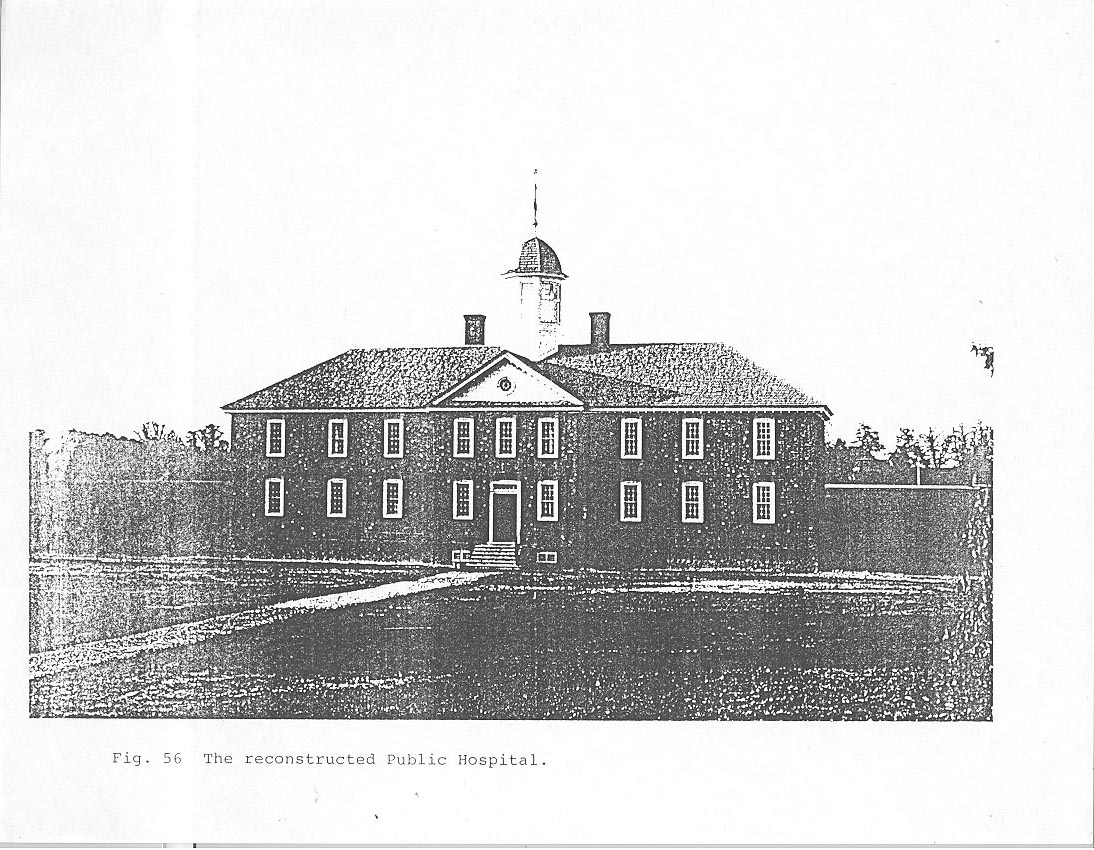 Fig. 56 The reconstructed Public Hospital.
"Description" and Benjamin Powell's contract, were used whenever possible. Other important sources were hospital records, historic visual material, and, as discussed earlier, archaeological findings. Certain items in each of these three categories were crucial to the reconstruction and served as constant research "touch stones." The 1974 Public Hospital research report by Gibbs and Rowe proved an indispensable source of documented facts. This rich compilation blended together material from legislative sources, administrative records, state treasurer's reports and receipts, the Virginia Gazette and other newspapers, insurance records, and miscellaneous papers of hospital trustees, directors and physicians. The most important documents in the visual category were two historic photographs of the hospital, showing the north elevation in 1869 and the south elevation in about 1885, and the 1829 drawing by keeper Dickie Galt, the project's "Bodleian Plate." The most significant archaeological "artifact" was, of course, the original hospital foundations.
Fig. 56 The reconstructed Public Hospital.
"Description" and Benjamin Powell's contract, were used whenever possible. Other important sources were hospital records, historic visual material, and, as discussed earlier, archaeological findings. Certain items in each of these three categories were crucial to the reconstruction and served as constant research "touch stones." The 1974 Public Hospital research report by Gibbs and Rowe proved an indispensable source of documented facts. This rich compilation blended together material from legislative sources, administrative records, state treasurer's reports and receipts, the Virginia Gazette and other newspapers, insurance records, and miscellaneous papers of hospital trustees, directors and physicians. The most important documents in the visual category were two historic photographs of the hospital, showing the north elevation in 1869 and the south elevation in about 1885, and the 1829 drawing by keeper Dickie Galt, the project's "Bodleian Plate." The most significant archaeological "artifact" was, of course, the original hospital foundations.
The committee decided that local original examples, rather than details from extant Robert Smith buildings in Philadelphia, should serve as prototypes for undocumented elements or details. Williamsburg buildings frequently consulted were the Courthouse of 1770, Bruton Parish Church tower, the Palmer House, the President's House, Brafferton Hall, and the Public Records Office. Buildings elsewhere in Virginia also served as sources for various details, specifically Carter's 76 Grove, the Nelson House, Berkeley, Shirley, Tuckahoe, Mt. Airy, Strawberry Hill, Blandfield and other buildings recorded as part of the Department of Architectural Research's ongoing fieldwork. Western State Hospital in Staunton became the principle source for the Hospital's nineteenth-century details.
BRICKWORK
The Public Hospital's reproduction brickwork is indicative of the many instances in which reliable factual information from archaeology, written documents, or illustrative documents had to be supplemented with additional comparative information. For example, Robert Smith's "Description" was relatively explicit concerning the brickwork for the hospital, providing an estimation of the total number of bricks (200,000), their size, and a calculation for measuring the number of bricks used in a "superficial foot" of finished wall. Yet, with the exception of the watertable, Smith left all decorative aspects such as arches, surrounds and beltcourse to the discretion of the local builder and bricklayer.
During the brickwork design process written documentation was first supplemented by even more specific information derived from archaeological excavation of the hospital foundations. An analysis of in situ brickwork established the average size of the brick (9" x 3" x 4 5/16"), 77 the color range, and the character of the mortar. Six different colors of red, brown, and plum brick were identified and constituted the next connector in the reconstruction process. By comparing the multi-colored original bricks to standing contemporary buildings in the vicinity, most notably the Courthouse (1770) and the Bruton Church tower (1769), the overall percentage of colors, the bonding and mortar quality, the color and quality of rubbed brick, and the color, texture, percentage, and distribution of random glazed brick were determined.7 As common as these features seem, they represent the subtle details by which buildings can be generally placed in local, regional and chronological context. A darker range of brick, with an equally dark shade of rubbed brick, evidenced by the extant Public Hospital bricks and the two above-mentioned buildings, is more characteristic of mid to late eighteenth-century brickwork in Williamsburg. Brick details above the watertable that were not documented in any way for the hospital, that is, rubbed surrounds, rubbed and gauged arches, and glazed brick, are decorative rather than functional design features. Such features, especially rubbed brick, were common in costly Virginia buildings of the eighteenth century. Their use began to decline after the Revolution and by the nineteenth century, few buildings featured glazed, rubbed, molded or gauged brick. Struck or lined joints, whose purpose was to provide a straight line in the irregular joint caused by uneven brick edges, also began to disappear in the nineteenth century as Federal period brickwork became more 78 refined. A good example of this decorative change can be seen at Bruton Church where the nave of the church built in 1715, displays a full pattern of glazed headers, while the tower, built in 1769, has a random pattern of partially glazed headers and stretchers. The hospital's brickwork was on the brink of these changes, reflecting a mid-to-late eighteenth-century style (Fig. 57).
Comparative analysis was not confined to the brick color. The brick bonding pattern, Flemish in combination with an English bond foundation, was easily established from local precedent. The mechanics of constructing a Flemish bond pattern, however, are typical only in a general manner, with the number of idiosyncratic examples equalled only by the number of different bricklayers who produced them. In a Flemish bond pattern, header and stretcher faces are laid so that they alternate both horizontally and vertically. The quality of handmade brick produces imperfect dimensions and an unpredictable factor in the horizontal dimension of a wall. Consequently, make-up bricks are inserted to help complete the horizontal row, especially between openings such as windows or doors. Make-up bricks can be either two or more contiguous headers or a combination of "clipped," shortened stretchers, usually three-quarters of their original size and generally referred to by bricklayers as "bats." The actual placement and type of make-up brick varies to the extent that it is rare to find a consistent pattern in a single building, much less from building to building. In effect, make-up
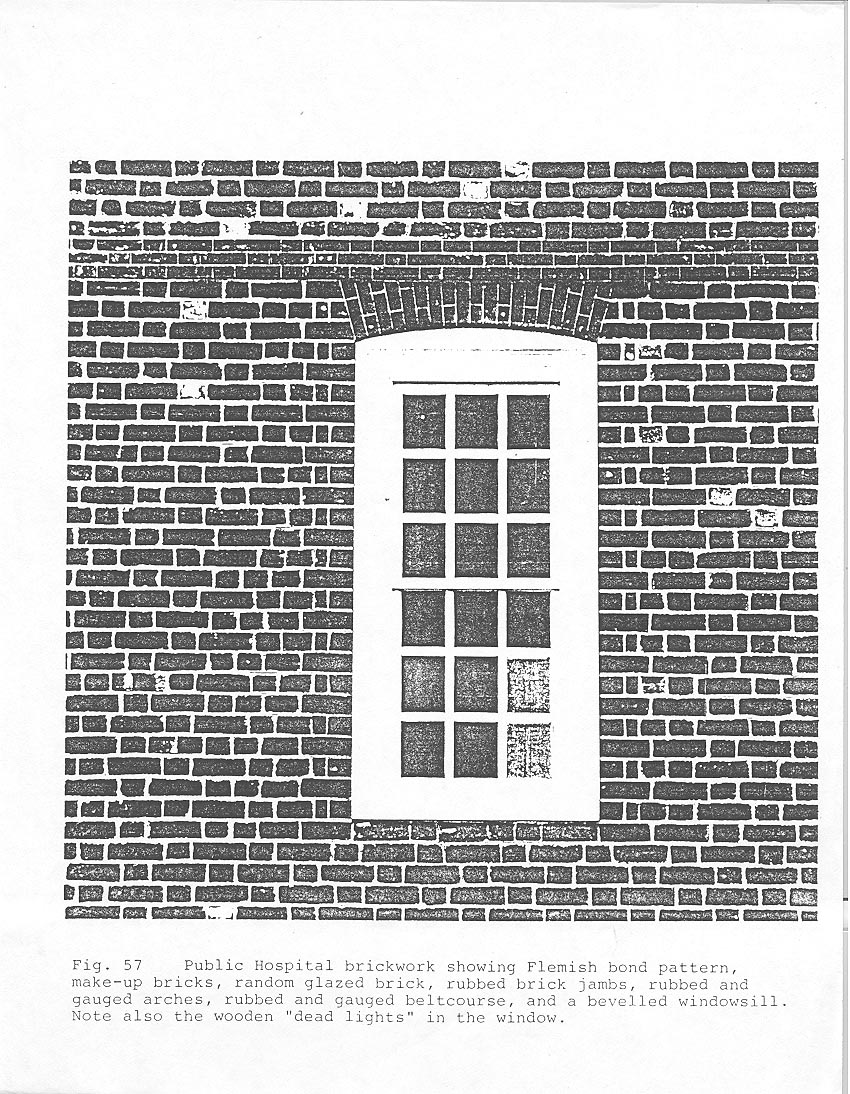 Fig. 57 Public Hospital brickwork showing Flemish bond pattern, make-up bricks, random glazed brick, rubbed brick jambs, rubbed and gauged arches, rubbed and gauged beltcourse, and a bevelled windowsill. Note also the wooden "dead lights" in the window.
79
bricks constitute a masonry signature reflecting a bricklayer's training and preference. Many modern reconstructions ignore the reality of make-up bricks, or when make-ups are used, they look far too similar and mechanical. Incorporating an authentic pattern of make-up bricks in the hospital's reconstructed brickwork was problematic. In order to replicate realistic patterns, the bricklayers were encouraged to make their own decisions about the use of a variety of documented options (Fig. 58). The result was unpredictable and, ultimately, more believable.
Fig. 57 Public Hospital brickwork showing Flemish bond pattern, make-up bricks, random glazed brick, rubbed brick jambs, rubbed and gauged arches, rubbed and gauged beltcourse, and a bevelled windowsill. Note also the wooden "dead lights" in the window.
79
bricks constitute a masonry signature reflecting a bricklayer's training and preference. Many modern reconstructions ignore the reality of make-up bricks, or when make-ups are used, they look far too similar and mechanical. Incorporating an authentic pattern of make-up bricks in the hospital's reconstructed brickwork was problematic. In order to replicate realistic patterns, the bricklayers were encouraged to make their own decisions about the use of a variety of documented options (Fig. 58). The result was unpredictable and, ultimately, more believable.
The actual reproduction of handmade brick proved formidable. Hand-molded bricks were fired in a manner that produced variations in color not only between bricks but within each individual brick. The basic colors were created in eight separate batches and then hand-blended according to the proper color-mix percentage. The bricks for corners, jambs, beltcourse, and arches required special preparations: screening for the right clay density, firing for a uniform color, and then precision cutting for their gauged size. Not only the masonry units and their pattern, but the material used for bonding received careful study. Over fifty experimental panels of mortar in varying combinations of sand, lime, shell, and cement were prepared and studied before achieving the proper color and texture (Fig. 59). A philosophical decision dictated that both the brick and the mortar resemble newly produced building materials, albeit
 Fig. 58 A bricklayer constructs a gauged arch with its tight "ptty" joints.
Fig. 58 A bricklayer constructs a gauged arch with its tight "ptty" joints.
 Fig. 59 Brick and shingle mock-ups were considered necessary for the first Colonial Williamsburg reconstructions (top) just as they were for the Publick Hospital (bottom).
80
eighteenth century in appearance, rather than instantly aged components as found in many earlier reconstructions.
Fig. 59 Brick and shingle mock-ups were considered necessary for the first Colonial Williamsburg reconstructions (top) just as they were for the Publick Hospital (bottom).
80
eighteenth century in appearance, rather than instantly aged components as found in many earlier reconstructions.
SHINGLES
Roof shingles represented another major effort to provide an authentic building material for the hospital. Although Robert Smith's "Description" did not mention the roof, Benjamin Powell's contract specified that it "be covered with plank and good Cypress Shingles." Heart cypress shingles, known for their longevity, were the most commonly used roof covering in Tidewater Virginia. The present-day lack of commercially produced heart cypress shingles forced a reliance on what turned out to be the most authentic product: traditional handmade shingles.
The characteristics and specifications for the shingles were based on eighteenth-century examples found in attics where they had dropped and been lost, on roofs that were later covered in place, and through early building contracts. Typically they measure 18" long, with 6" exposed to the weather, ½" to ¾" thick at the butt, 3" to 5" wide, and tapered to a thin edge at the top.
The effort to produce a single shingle is a rather long and involved one. Cypress logs ranging from 20" to 40" in diameter were first individually selected for suitable characteristics. After cutting the logs into 18" sections, the 81 outer ring of sapwood was split off with a sledge hammer and wedges and thrown away. The remaining heartwood was then split into billets. These billets were further reduced by a froe and club into rough shakes. Each shake was then placed on a specially adapted shaving horse and tapered, planed, and rounded on the butt end by craftsmen using drawknives and other tools to produce a final, smoothly finished shingle (Fig.60). Total production was impressive and time consuming: 2 to 4 people working for about a year produced over 30,000 shingles. But that was not the end of each shingle's special handling. For certain parts of the hipped roof, such as the ridges and valleys, each shingle had to be carefully cut with hatchets and planes to form fantail or swept valley pieces (Fig. 61). The most skillful work was needed for the cupola roof where each shingle had to be cut and fitted for a two directional curve.
STONE STEPS
In some cases, documentary evidence combined with a degree of deductive reasoning advanced the design process. For instance, the stone steps were among the building materials imported from England. Robert Carter Nicholas ordered the steps from John Norton and Sons in London in 1772: "I trouble you with a Letter for Mr. Saml. Martin of Whitehaven, it is to desire the favour of him to send over some Stone Steps for an Hospital the
 A shingle craftsman working on a shaving horse tapers a rough cypress shake into a finished shingle with the use of a drawknife
A shingle craftsman working on a shaving horse tapers a rough cypress shake into a finished shingle with the use of a drawknife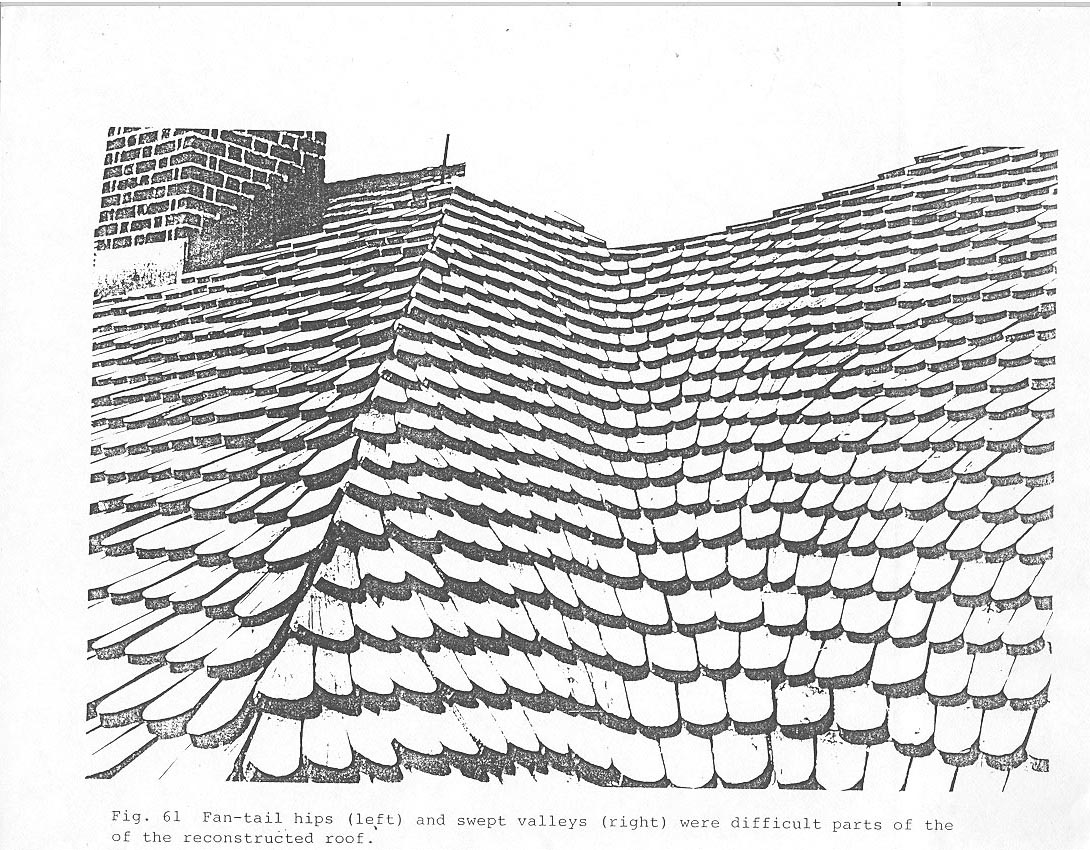 Fig. 61 Fan-tail hips (left) and swept valleys (right) were difficult parts of the reconstructed roof.82
Country is building for the Reception of Lunaticks & other unhappy objects of insane Minds, which it is fear'd will multiply too fast in this Country…."8 Efforts to find specific documentation was futile, except for the price paid for the stone. An analysis of contemporary prices of stone in England, colonial exchange rates, and the estimated size of the hospital steps suggested that enough stone was available for the north and south steps, but not for those on the east and west. Hence the principal north and south steps were reconstructed in stone and the secondary east and west stairs in wood, with details for both stone and wood steps taken from appropriate local original examples (Fig. 62).
Fig. 61 Fan-tail hips (left) and swept valleys (right) were difficult parts of the reconstructed roof.82
Country is building for the Reception of Lunaticks & other unhappy objects of insane Minds, which it is fear'd will multiply too fast in this Country…."8 Efforts to find specific documentation was futile, except for the price paid for the stone. An analysis of contemporary prices of stone in England, colonial exchange rates, and the estimated size of the hospital steps suggested that enough stone was available for the north and south steps, but not for those on the east and west. Hence the principal north and south steps were reconstructed in stone and the secondary east and west stairs in wood, with details for both stone and wood steps taken from appropriate local original examples (Fig. 62).
EXTERIOR TRIM
Keeper Dickie Galt's 1829 drawing of the hospital proved to be a source for many details but like written documentary sources, this too had to be supplemented with additional information. Benjamin Powell's contract called for a "neat Mundelian Cornice" and for a "neat Pediment" on the north of the building. Both of these features can be seen in the Galt drawing, which shows a modillian cornice and a pediment with a raked modillion cornice, lower tympanum weathering, and a round window centered in the tympanum. A close examination of the 1869 and 1885 photographs of the hospital indicated that the original
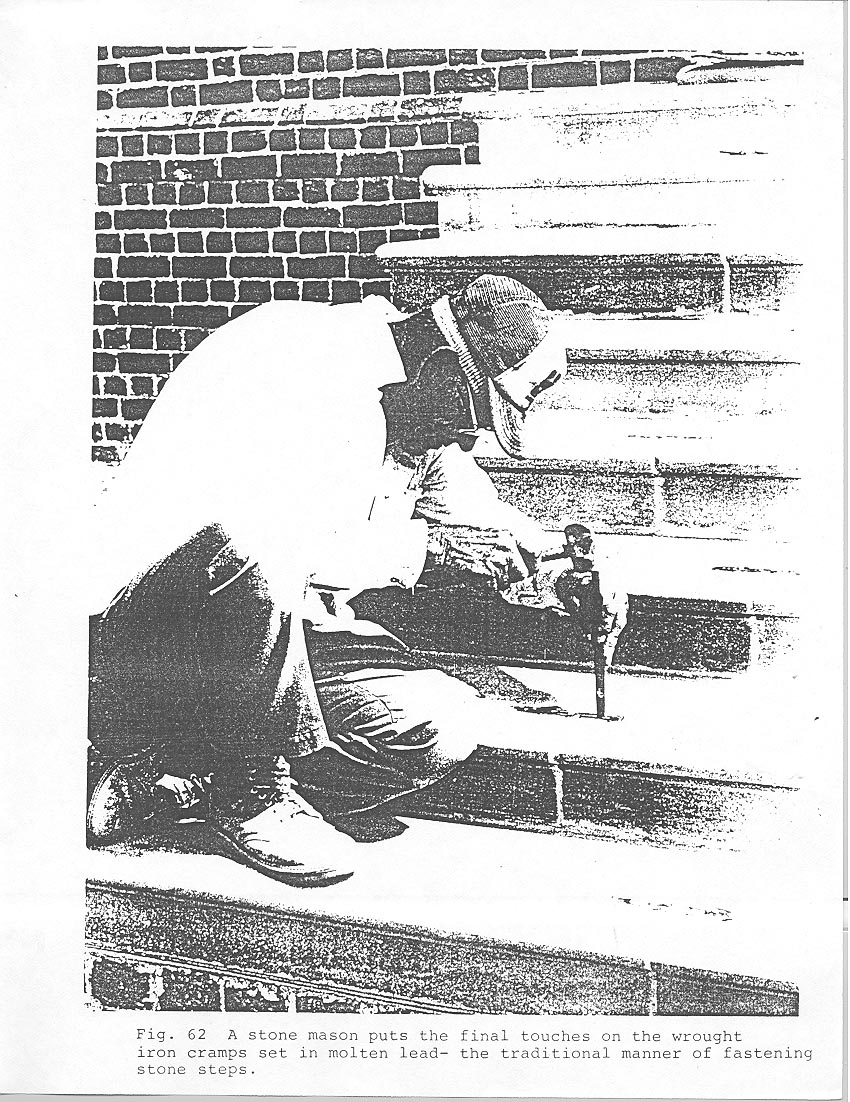 Fig. 62 A stone mason puts the final touches on the wrought iron cramps set in molten lead, the traditional manner of fastening stone steps.
83
cornice and pediment had probably been reused when the cornice and roof were raised for a third floor addition. The original pediment had, in fact, been displaced by a massive Greek Revival portico on the front of the building and reinstalled on the back. The clue to this relocation was the unmistakable Georgian scale of the cornice and pediment in diminutive contrast to the Greek Revival details.
Fig. 62 A stone mason puts the final touches on the wrought iron cramps set in molten lead, the traditional manner of fastening stone steps.
83
cornice and pediment had probably been reused when the cornice and roof were raised for a third floor addition. The original pediment had, in fact, been displaced by a massive Greek Revival portico on the front of the building and reinstalled on the back. The clue to this relocation was the unmistakable Georgian scale of the cornice and pediment in diminutive contrast to the Greek Revival details.
CUPOLA
Neither Robert Smith nor Benjamin Powell mentioned the hospital's cupola and weathervane (Fig. 63). Cupolas were associated with public buildings in eighteenth-century America, and, considering his reliance on a standard institutional form, it was natural for Robert Smith to design one for the Public Hospital. The Galt drawing does, in fact, show a cupola and some of its details. Accounts for repairs in 1803,1808, and 1817 provided even more details for a reconstructed design. For its overall size and shape, however, contemporary examples were compared, since it was determined that the cupola as depicted by Dickie Galt was slightly exaggerated. With reference to Robert Smith's cupola designs, a clear evolution in form was observed reflecting a more widespread stylistic trend. The flared, angular, bell-cast cupola roof forms found earlier in the eighteenth century give way to those more rounded and
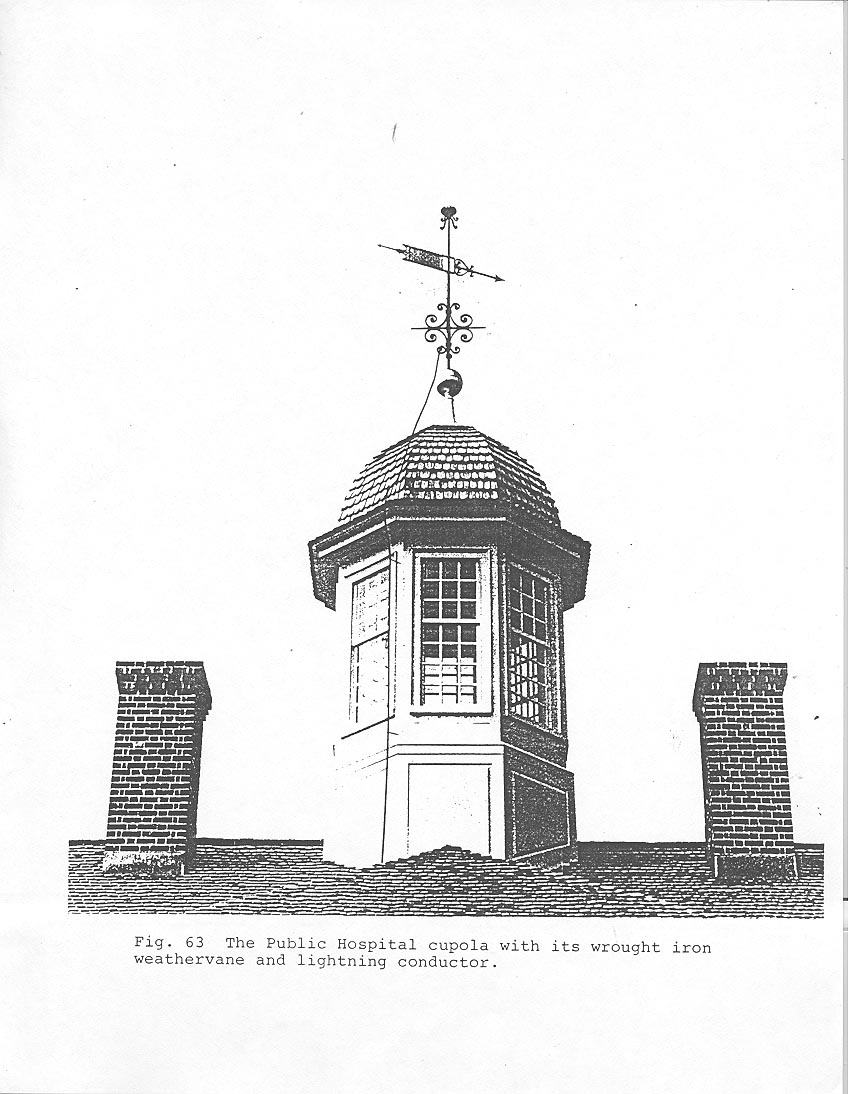 Fig. 63 The Public Hospital cupola with its wrought iron weathervane and lightning conductor.
84
neo-classical in appearance later in the century. In Williamsburg there is an obvious transition from the tall, narrow, tiered cupolas of the early eighteenth century, as seen in the Capitol (1701), the Palace (1706) and the Wren Building (1716), to those later in the century at the Courthouse (1770) and the hospital. It was a similar evolution in aesthetic taste that led to the demise of the hospital's original cupola. After first stating that the original cupola would be reused in the new third-story roof in 1840, the hospital's building committee reconsidered and felt that "the old cupola [was] much too small to be congruous with the enlarged building; and thought that a larger one of a different description would be necessary to answer the only end for which a cupola was at all intended - Vis. that of ornament." The drawing "submitted by the principal carpenter" was for the Greek Revival cupola recorded in the 1885 photograph of the south elevation.
Fig. 63 The Public Hospital cupola with its wrought iron weathervane and lightning conductor.
84
neo-classical in appearance later in the century. In Williamsburg there is an obvious transition from the tall, narrow, tiered cupolas of the early eighteenth century, as seen in the Capitol (1701), the Palace (1706) and the Wren Building (1716), to those later in the century at the Courthouse (1770) and the hospital. It was a similar evolution in aesthetic taste that led to the demise of the hospital's original cupola. After first stating that the original cupola would be reused in the new third-story roof in 1840, the hospital's building committee reconsidered and felt that "the old cupola [was] much too small to be congruous with the enlarged building; and thought that a larger one of a different description would be necessary to answer the only end for which a cupola was at all intended - Vis. that of ornament." The drawing "submitted by the principal carpenter" was for the Greek Revival cupola recorded in the 1885 photograph of the south elevation.
WEATHERVANE
The hospital's weathervane, also represented in the Galt drawing, was further documented through William Nelson's letters of protest to London merchant Robert Cary in 1771. Upon seeing the imported vane, Benjamin Powell felt that Nelson had been overcharged, prompting Nelson's letters to Cary in which he mentions certain parts of the vane.9 Later repair accounts 85 mention still other parts of the vane. For details, American and English weathervanes of the same period were used as prototypes in designing the reconstructed vane. The Williamsburg Courthouse which retains its original weathervane, became the principal source of construction details. Like the evolution in cupolas, weathervanes also changed over time. The banner type vane of the Governor's Palace, representing early eighteenth-century forms, can be compared to the later banneret forms of Bruton Parish Church, the Courthouse and the Hospital. Forged of wrought iron, the reconstructed hospital vane was handmade by Colonial Williamsburg blacksmiths (Fig. 64). The hollow copper ball, hammered from flat sheets into two spheres by the master silversmith and covered in gold leaf, contains commemorative objects placed there in continuation of an ancient tradition (Fig. 65). This tradition dates to as early as the thirteenth century when the ball of the weathervane at St. Paul's Cathedral in London "was filled with relics of saints destined to protect it from storms, and these were examined and renewed from time to time with much ceremoney."10 More indigenous examples come from Faneuil Hall and Christ Church in Boston.11
LIGHTNING CONDUCTOR
Comparative evidence and prototypes were important for two other exterior elements: the lightning conductor and the
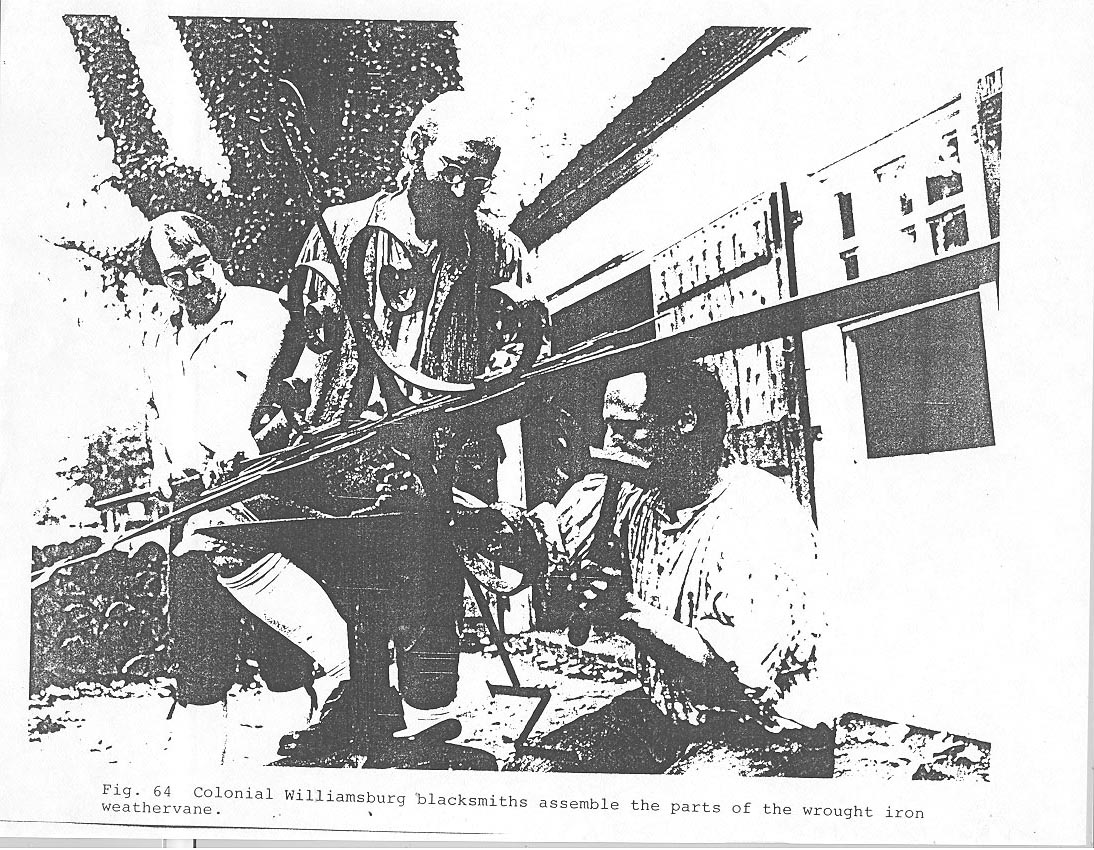 Fig. 64 Colonial Williamsburg blacksmiths assemble the parts of the wrought iron weathervane.
Fig. 64 Colonial Williamsburg blacksmiths assemble the parts of the wrought iron weathervane.
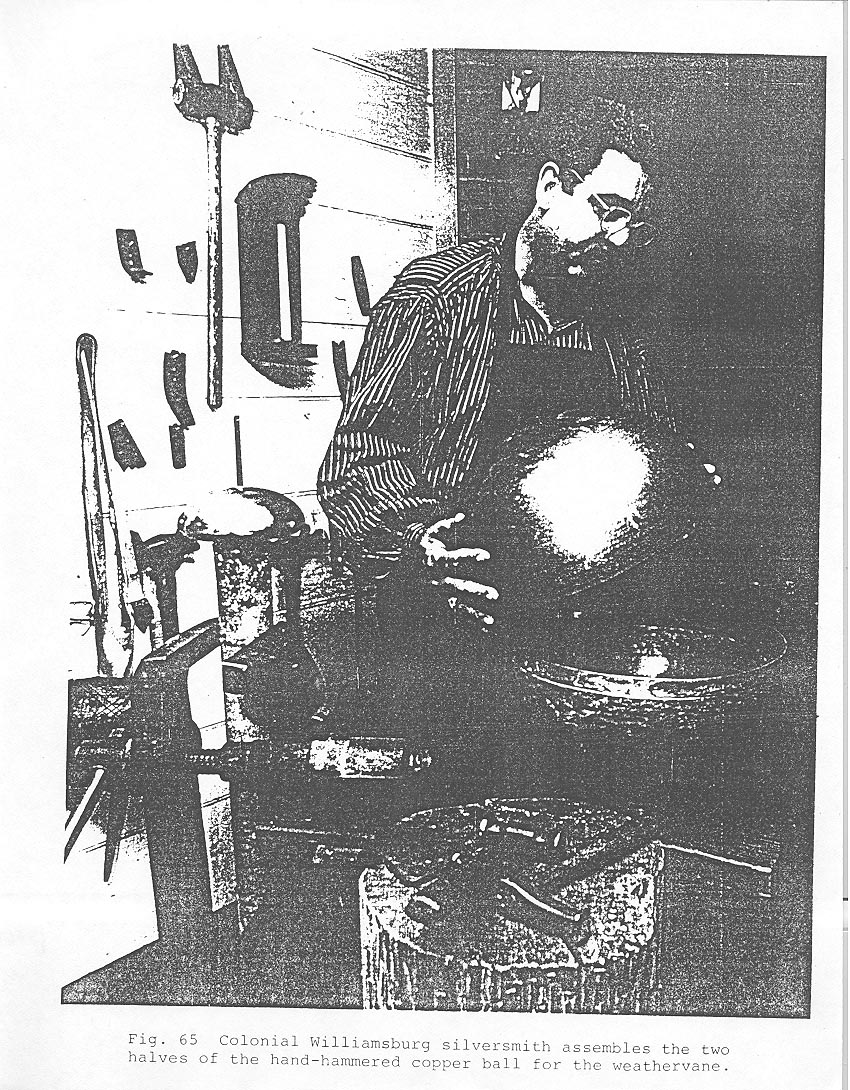 Fig. 65 Colonial Williamsburg silversmith assembles the two halves of the hand-hammered copper ball for the weathervane.
86
exercise yard fence. The hospital's lightning conductor ground
had been uncovered next to the foundation wall. There was no reason to suspect that a lightning conductor was not an original part of the building in 1773. Its anchor spikes soundly driven into the clay subsoil indicated that the piece had not been moved since installation. The principal evidence for this assumption was an account of blacksmith James Anderson in 1789. Among the repairs and work at the hospital recorded in Anderson's ledger for that year is the entry for taking down, altering, and reinstalling a lightning conductor.12 Original construction records do not survive but the absence of any references to a new hospital conductor in Anderson's 1778-1785 ledger makes it likely that the lightning conductor was placed on the building at its completion. To substantiate that the conductor ground was indeed an eighteenth-century form and to find further design evidence for the reconstructed conductor, research was conducted on surviving conductors in Williamsburg, in Virginia and in the region.13 The ground was found to be very similar to others in the area, including one at Bruton Parish Church, Tazewell Hall, and Kingsmill. Lightning conductors were very common in Williamsburg and Virginia by the 1770s. The first known reference to their use in Virginia is remarkably early: 1752, only three years after Benjamin Franklin installed a conductor on his own house. By 1781 a French traveller in Williamsburg reported that "Upon nearly all the houses are lightning rods (conducteurs)."14 A few years later, a German traveller's description of Virginia
87
stated that "…the people generally have spared neither cost nor trouble in protecting their houses by electric conductors, that beneficent discovery of the great Franklin. One fails to see them almost nowhere in the great towns or on the larger houses in the country.15
Fig. 65 Colonial Williamsburg silversmith assembles the two halves of the hand-hammered copper ball for the weathervane.
86
exercise yard fence. The hospital's lightning conductor ground
had been uncovered next to the foundation wall. There was no reason to suspect that a lightning conductor was not an original part of the building in 1773. Its anchor spikes soundly driven into the clay subsoil indicated that the piece had not been moved since installation. The principal evidence for this assumption was an account of blacksmith James Anderson in 1789. Among the repairs and work at the hospital recorded in Anderson's ledger for that year is the entry for taking down, altering, and reinstalling a lightning conductor.12 Original construction records do not survive but the absence of any references to a new hospital conductor in Anderson's 1778-1785 ledger makes it likely that the lightning conductor was placed on the building at its completion. To substantiate that the conductor ground was indeed an eighteenth-century form and to find further design evidence for the reconstructed conductor, research was conducted on surviving conductors in Williamsburg, in Virginia and in the region.13 The ground was found to be very similar to others in the area, including one at Bruton Parish Church, Tazewell Hall, and Kingsmill. Lightning conductors were very common in Williamsburg and Virginia by the 1770s. The first known reference to their use in Virginia is remarkably early: 1752, only three years after Benjamin Franklin installed a conductor on his own house. By 1781 a French traveller in Williamsburg reported that "Upon nearly all the houses are lightning rods (conducteurs)."14 A few years later, a German traveller's description of Virginia
87
stated that "…the people generally have spared neither cost nor trouble in protecting their houses by electric conductors, that beneficent discovery of the great Franklin. One fails to see them almost nowhere in the great towns or on the larger houses in the country.15
Based on well preserved examples, the hospital's reconstructed conductor is composed on rounded bars of iron wrought together to form a continuous piece from the connecting ground link to the base of the cupola (Fig. 66). At the top, the conductor is attached to the shaft of the Weathervane, which, in effect, acts as the conductors top point. The historic 1885 photograph of the hospital shows a replacement conductor leading to the Greek Revival cupola but still using the original ground. It was common in the nineteenth century for wrought iron conductors to be replaced by flexible braided wire, which was often installed without regard to the building's roof line, as many old photographs indicate.
EXERCISE YARD FENCES
More rare than surviving eighteenth-century lightning conductors are exercise yard fences. Wooden fences were understandably short lived. Archaeological evidence provided the post hole locations for the east exercise yard and for part of the west yard (Fig. 67), but the structural features of such a
 [illegible]
[illegible]
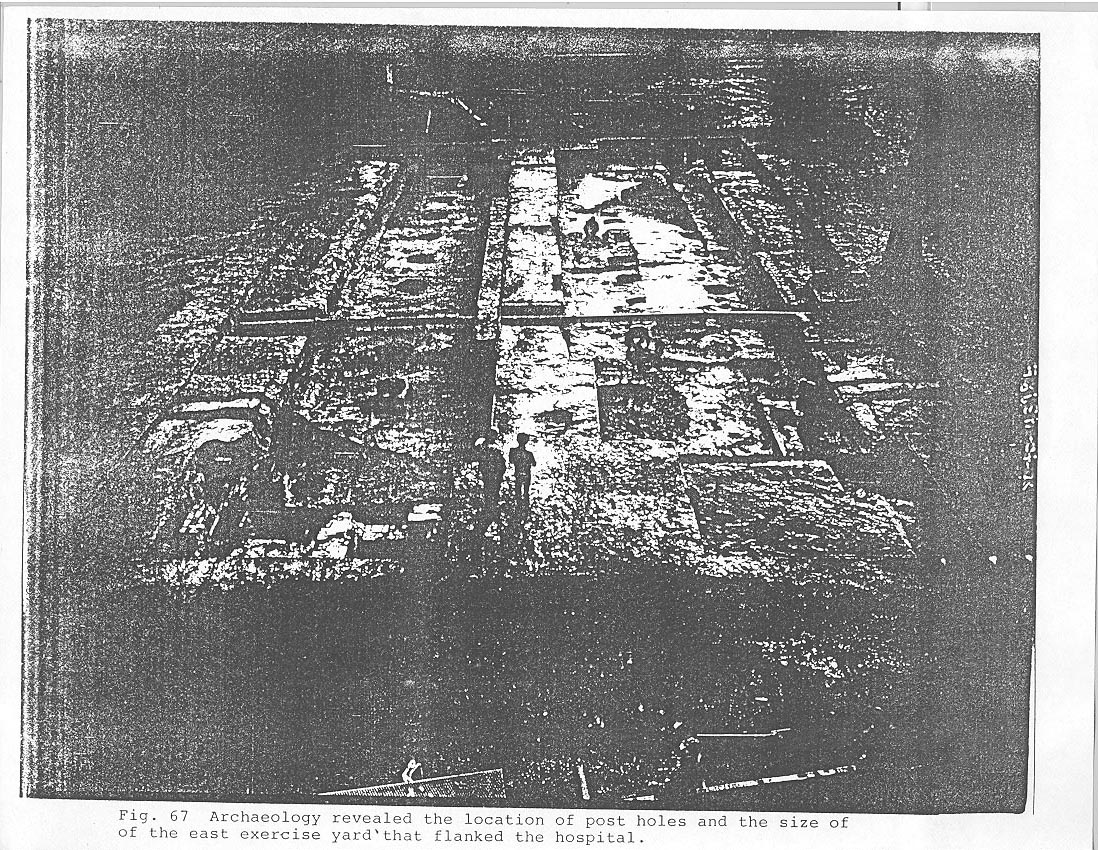 Fig. 67 Archaeology revealed the location of post holes and the size of the east exercise yard that flanked the hospital.
88
fence were much harder to document. Logic called for the fence to be constructed inside-out, with the rails on the outside to prevent escape. This arrangement was confirmed by illustrations of analogous almshouse fences. Details for construction were derived from written specifications for jail and almshouse fences, most significantly the description of an 11' high Richmond Poor House exercise yard fence that gave exact dimensions for all of its parts.16 The east yard of the hospital is interpreted as a barren space, since there were no documented structures in the yards before 1800.
Fig. 67 Archaeology revealed the location of post holes and the size of the east exercise yard that flanked the hospital.
88
fence were much harder to document. Logic called for the fence to be constructed inside-out, with the rails on the outside to prevent escape. This arrangement was confirmed by illustrations of analogous almshouse fences. Details for construction were derived from written specifications for jail and almshouse fences, most significantly the description of an 11' high Richmond Poor House exercise yard fence that gave exact dimensions for all of its parts.16 The east yard of the hospital is interpreted as a barren space, since there were no documented structures in the yards before 1800.
INTERIOR RECONSTRUCTION
Interior reconstruction at the Public Hospital is confined to the east wing of the first floor and within that wing to a portion of the north range of cells and to the central passage. Rather than interpreting a number of redundant eighteenth-century cells, the hospital departs from the predominant interpretive philosophy of the Historic Area by the inclusion of a nineteenth-century room. The hospital's most significant historical period lies in its founding. Perhaps the most interesting historical aspect of this institution, however, is what became of that beginning, and how it relates to our understanding of the modern practice of psychiatry. The extremely 89 rich collection of nineteenth-century Eastern State Hospital documents, especially those of the Galt family, and the extant examples of contemporary hospitals throughout the country make the inclusion of the hospital's nineteenth-century history a rare opportunity to interpret a significant era of medicine. Similarly, it was felt that rather than interpreting more than one post-colonial patient room, the space might be better used for telling a more complete story, one that could not be conveyed solely by reconstructed rooms or through published works. Consequently, the area south of the east Wing passage, the space once occupied by three eighteenth-century cells, contains a modern exhibit space that concisely documents the changes over time from 1773 to 1885, the year the original building burned. This 102 year history is told in three segments: the Age of Restraint, 1773-1835; the Moral Management Era, 1836-1862; and the Custodial-Care Regime, 1862-1885. Two reconstructed cells represent the first and second periods in this time span.
To reconstruct any part of the interior it was necessary to understand the configuration of the original plan, how the building had been used and by whom, and whether the arrangement of space and its finish had been altered over time. The interior was conceived as a number of zones defined by function and circulation. In each zone there existed a corresponding level of detail and finish. For example, such spaces as the entry hall and the directors' room typically had a high level of finish, including perhaps a panelled wainscot and 90 plaster walls. In the passages and in the patient's cells, a less finished treatment prevailed. The same hierarchy applies to other details such as door and window moldings. In other words, the smallest detail, and its location, seemingly common and explicit, conveys meaning and inherent social values. The theoretical and analytical basis for this system emerged largely from Colonial Williamsburg's architectural fieldwork, which seeks to document through measured drawings, photographs, and documentary research quickly vanishing eighteenth and early nineteenth-century structures in the Tidewater region. Documentation of specific building types relevant to the hospital, such as jails, almshouses, and asylums augmented the design research. A conscientious effort was made to use local or regional examples when possible, although part of the significance of hospital design in the Moral Management era of the nineteenth century was the standardized and even international use of common architectural forms and details.
The east wing interior passage, with its six cell doors, is reconstructed to its earliest eighteenth-century appearance (Fig. 68). Its represents one of four nearly identical passages on the first and second floors of the hospital. By analyzing an account for plaster work in 1776, it was determined that the passages, but not the cells, were probably fully plastered. In terms of details, the passages were less finished than the more public areas of the building, but superior to that of the cells. Such hierarchy of building finishes is displayed in
 Fig. 68 The reconstructed passage with its six cell doors .
Fig. 68 The reconstructed passage with its six cell doors .
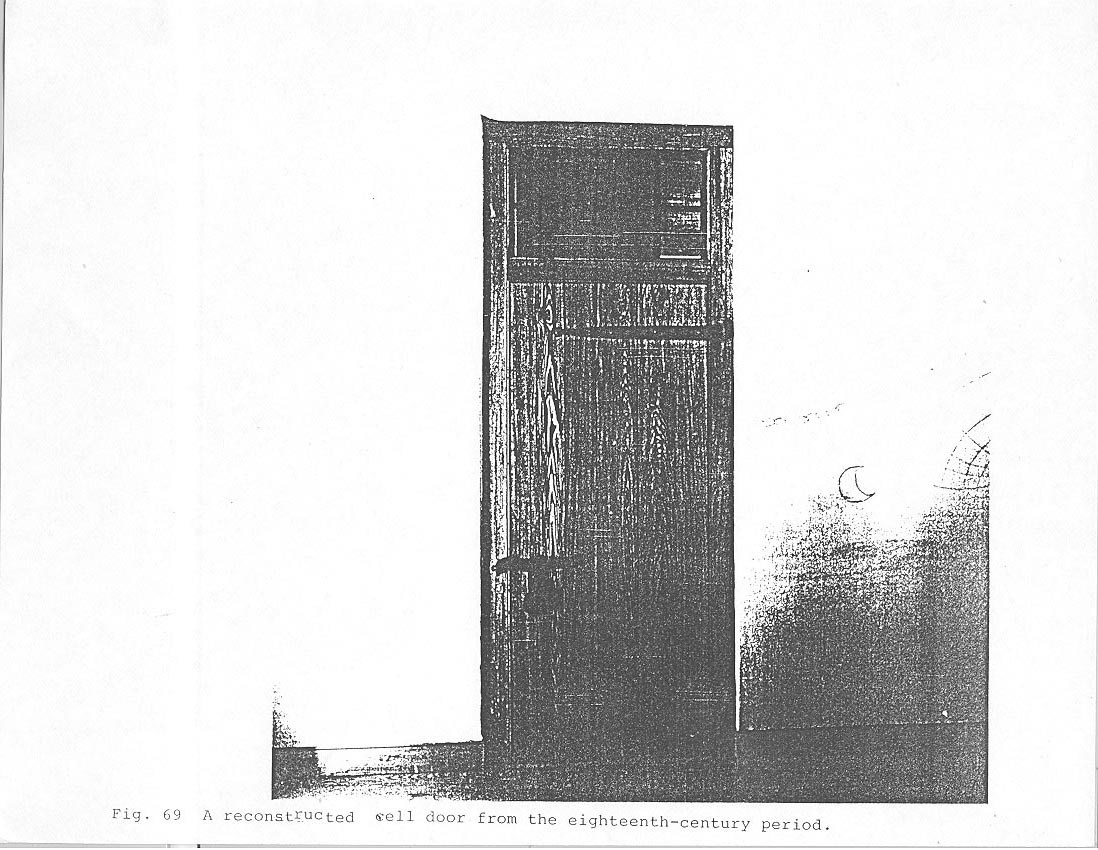 Fig. 69 A reconstructed well door from the eighteenth-century period.
Fig. 69 A reconstructed well door from the eighteenth-century period.
 Fig. 70 The reconstructed eighteenth-century patient cell.
Fig. 70 The reconstructed eighteenth-century patient cell.
 Fig. 71 Robert Smith sketches copied into the Directors' Minute Book showing the elevation (top) and plan (bottom) of the window grate.
91
door trim, among other details, where the complexity of moldings depends upon which side of the door is the more public.
Fig. 71 Robert Smith sketches copied into the Directors' Minute Book showing the elevation (top) and plan (bottom) of the window grate.
91
door trim, among other details, where the complexity of moldings depends upon which side of the door is the more public.
Specific documentation for the interior finish and appearance of the early cells was scarce. In the earliest period, one of the most frequent references to cell finish is that of whitewashing. The plain window and door casings, the plank ceiling and the exposed English bond wall reflect a lower scale of finish analogous to work and storage spaces or to slave quarters (Fig. 69). Eighteenth-century illustrations of hospitals for the insane, such as William Hogarth's depiction of the interior of Bedlam Hospital, provided both the documentation and the source for various forms of patient graffitti, which appears at the Public Hospital.
Benjamin Powell's building contract specified "strong batten Doors" for the hospital cells. Board-and-batten doors were traditionally used for areas of greatest security. The passage doors, on the other hand, are of double thickness, with panels on one side and sheathed boards on the other, expressing concern for appearance as well as security. Even though some patients were confined in leg or wrist chains, the doors were well secured by locks and bolts (Fig. 70).
Robert Smith took great care to. specify the interior window grates. His "Description" included two sketches showing in plan and elevation what they were to look like and exactly how the grates were to be mounted in the brick wall (Fig. 71). The window bars did not prevent patients from breaking glass out of
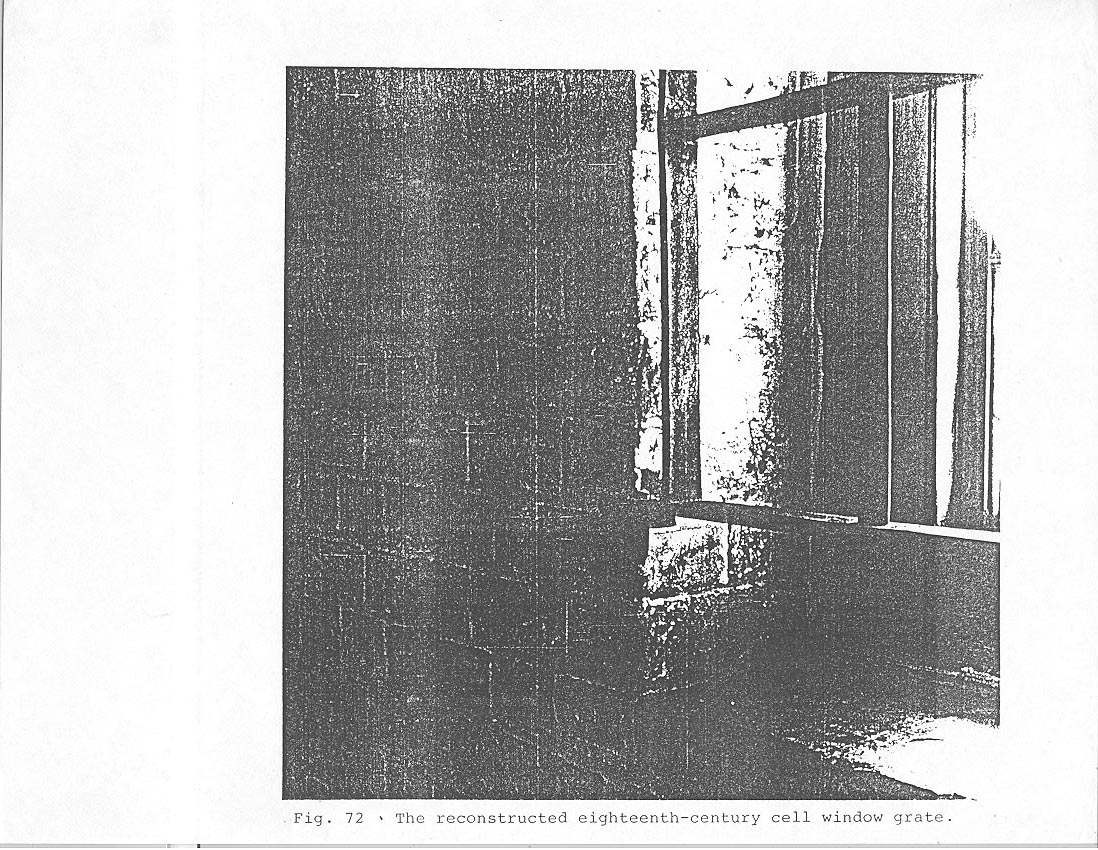 Fig. 72 The reconstructed eighteenth-century cell window grate.
Fig. 72 The reconstructed eighteenth-century cell window grate.
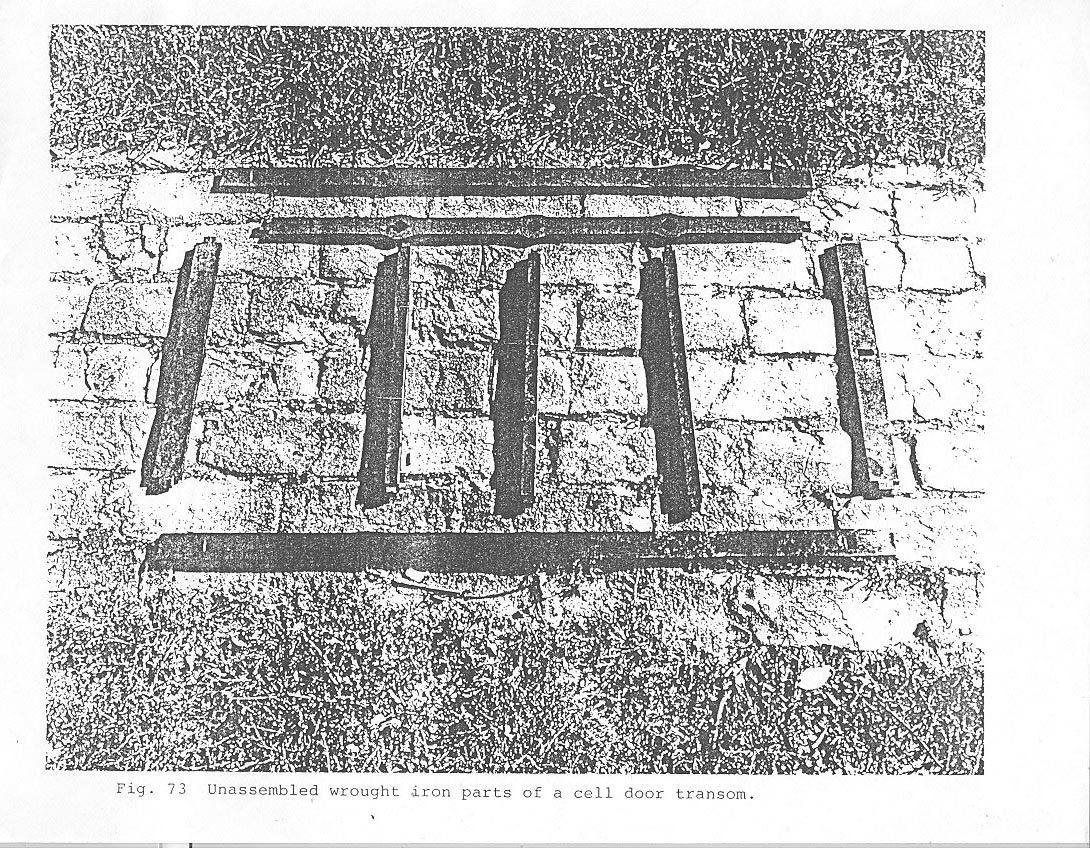 Fig. 73 Unassembled wrought iron parts of a cell door transom.
92
the windows, which the keeper sometimes replaced with wooden "dead lights" rather than glass. The wrought iron window grate and transoms, like the chains, locks, bolts, hinges, and nails were all forged by Colonial Williamsburg blacksmiths (Fig. 72). Director Robert Carter's order for 48 grates from the Baltimore -Iron Works in 1771 specified that "…24 of the larger size and 24 of the other size are wanted, both sizes to be made of wroght iron…." This reference to smaller grates is interpreted as describing transoms over the doors, based on examples commonly used in eighteenth-century European and American jails, asylums, at the Pennsylvania Hospital,-and at the 1820 Public Hospital additions (Fig.73).
Fig. 73 Unassembled wrought iron parts of a cell door transom.
92
the windows, which the keeper sometimes replaced with wooden "dead lights" rather than glass. The wrought iron window grate and transoms, like the chains, locks, bolts, hinges, and nails were all forged by Colonial Williamsburg blacksmiths (Fig. 72). Director Robert Carter's order for 48 grates from the Baltimore -Iron Works in 1771 specified that "…24 of the larger size and 24 of the other size are wanted, both sizes to be made of wroght iron…." This reference to smaller grates is interpreted as describing transoms over the doors, based on examples commonly used in eighteenth-century European and American jails, asylums, at the Pennsylvania Hospital,-and at the 1820 Public Hospital additions (Fig.73).
Spare and grim, the cells in the Public Hospital offered no amenities to patients who were frequently chained to the wall. Winter suits of clothing and blankets offered a minimum of comfort in the unheated cells. Fireplaces appeared only in the cellar kitchen, the first floor keeper's quarters, and the second floor directors' room. In the eighteenth century it was customary to provide unheated institutional spaces for the insane, paupers or criminals. The Pennsylvania Hospital warmed its cellar cells with stoves, which probably prompted Robert Smith to include this suggestion in his "Description:" "If there shou'd be occasion for Fire to warm the common Rooms, there may be Stoves fixed in the Partition between two Rooms with the Mouth open to the Passage, by which means they make fires and the mad People cannot come at them. They should be fixed about two foot
93open to the Passage, by which means they make fires and the mad people cannot come at them. They shou'd be fixed about two foot
above the floor for fear of the Patients falling against the Stoves." These stoves were never installed in the Williamsburg hospital and as late as the 1830s it was reported that the patients obtained warmth only by gathering during the day in common rooms near a fireplace.
The 1845 "apartment," as the patients' rooms were then called, represents the environmental change that took place at the hospital with the advent of Moral Management treatment under Dr. John M. Galt II. The physical change purposefully created a more normal domestic setting: screened transoms replaced bars, plaster covered the brick walls, windows and doors were more decoratively treated, and exterior cast iron sash replaced the interior jail-like grates (Fig. 74). The latter element became one of the most widely used architectural features in nineteenth-century asylums, having been recommended by Samuel Tuke in his influential Description of the Retreat in 1813 and in later treatises. John Conolly in The Construction and Government of Lunatic Asylums and Hospitals for the Insane, published in 1847, succinctly stated the new goal of asylum building: "The recovery of the curable, the improvement of the incurable, the comfort and happiness of all the patients, should therefore steadily be kept in view by the architect from the moment in which he commences his plan…."
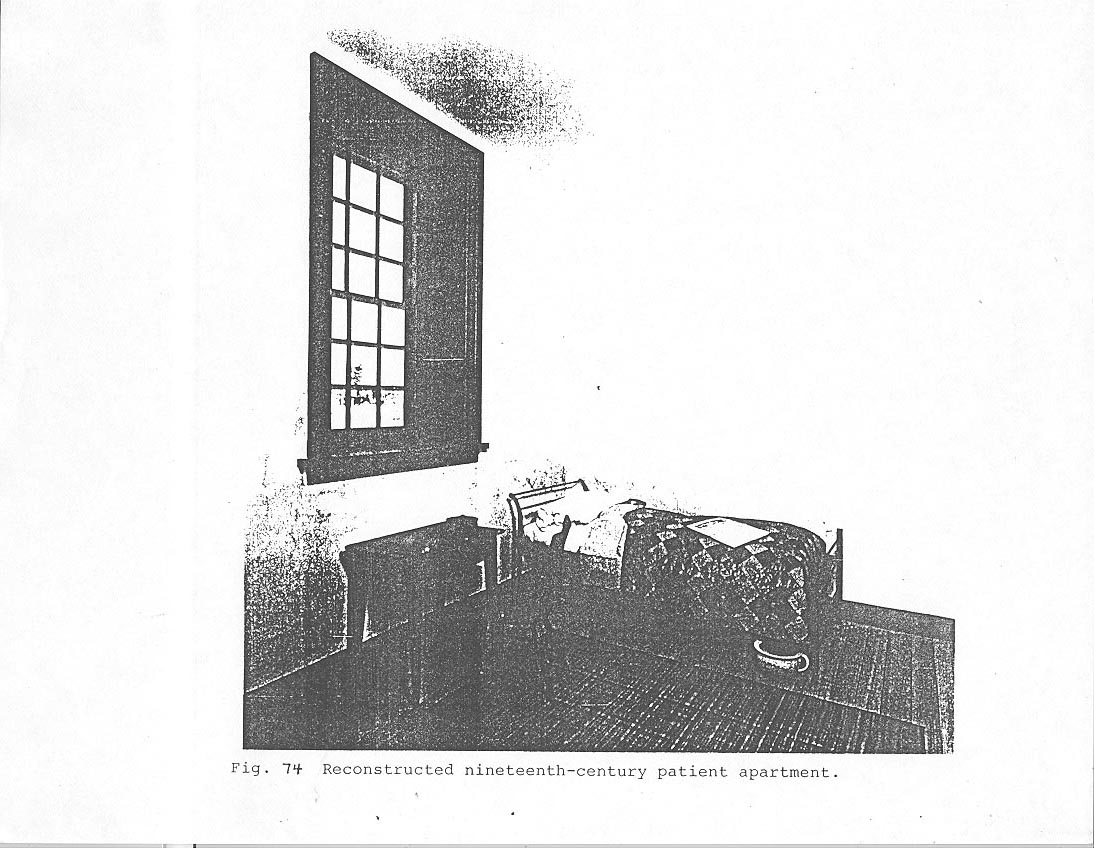 Fig. 74 Reconstructed nineteenth-century patient apartment.
94
are documented in an 1840 change order for the third floor addition to the original Public Hospital building and its west wing. The iron bed was reproduced from examples that survived the building's destruction. Cast iron sash have not been reconstructed because they were attached to the exterior of the window and the hospital's reconstructed exterior represents an eighteenth-century appearance. Graffitti in this room was reproduced directly from patients' letters and diaries.
Fig. 74 Reconstructed nineteenth-century patient apartment.
94
are documented in an 1840 change order for the third floor addition to the original Public Hospital building and its west wing. The iron bed was reproduced from examples that survived the building's destruction. Cast iron sash have not been reconstructed because they were attached to the exterior of the window and the hospital's reconstructed exterior represents an eighteenth-century appearance. Graffitti in this room was reproduced directly from patients' letters and diaries.
CHAPTER VIII
NOTES
September 5, 1771
The Invoice of the Cross, vane & ca amounting to £27.14..- which is received & I credit you for it in Account, but the Builder says, that it is most extravagantly dear, & that he had one made here nearly as Good for £12 our Currency, tho' the spindle is not turned, as this is; and therefore, if no Abatement is made, I shall think they take a very unfair Advantage of Charging what they please for their goods.Novermber 21, 1771
I hope you will try to get some Allowance for the Excessive Charge of the Weather Cock, which I complain'd of before or I shall think hardly dealt by.February 21, 1772
I observe the Reasons, which Mr. Millington gives for the high price of the Vane & Ca. which I suppose I must be satisfied with tho not convinced that it was not too Dear.
The famous grasshopper vane by Shem Downe suffered several mishaps, including a fall from the steeple caused by the 1755 earthquake and another fall in 1889. During one of the repairs related to these accidents the grasshopper was found to have a "vest pocket" in which was found a paper with the following history: "Shem Downe made it May 25, 1742. To my brethren and fellow Grasshopper: Fell in ye year 1753 Nov. 18, early in ye morning by a great earthquake by my Old Master above… Again Like to have met with my Utter Ruin by fire, but hopping timely from by Public Situation came off with Broken bones and much Bruised Cured and fixed…[by] Old Master's son Thomas Downe June 28, 1768, and though I will promise to Discharge by Office, yet I shall vary as ye wind.
Mrs. Samuel G. Babcock, "The Weather Vane of Christ Church, Boston," Old Time New England, October 1941. Reverend William Croswell wrote in his diary in 1834 when the vane was repaired that he "wrote something to put in the ball of the 97 steeple, arranged in the shape of a cross." The same steeple and vane was repaired in 1934, at which time "a sodden mass of papers," thought to date from an 1847 repair, were removed from the ball and new documents were once again sealed in the ball.
"…a plank enclosure of about 310 feet in length, the posts to be 14 feet long, 10 feet of each post to be hewed squre, at the bottom of the square, to be 9 inches, and at top, 6 inches square, of good white or post oak, the pannels to be 8 feet long, 4 rails of good white oak to each panel, the rails to be 4 by 2 ½ inches and 16 ½ feet long, to embrace 3 posts each, the whole of said plank enclosure to be surmounted with an oak railing of 4 inches by 1 ¼, with 20d nails projecting through said railing at one inch distance from each other…."
APPENDIX A
ROBERT SMITH'S SPECIFICATIONS FOR THE PUBLIC HOSPITAL
A Description of the Plan and Elevation of A Hospital for Virginia
The Plan consists of a Hall for a Staircase, behind There is the Keepers apartment, and 12 other Rooms chiefly for the Reception of mad People. The Stairs begin near the front Door and lands on [?] passage in the second Story. The second Story has 12 Rooms the same Dimensions as those in the first Story, and a Room over the Keepers Apartment which may serve the Managers of the Hospital to meet or may be divided which will make two other Rooms for Patients. The Hall is designed to be open as far as the landing of the Stairs the whole hight of both Storys. The cellers, shoud be about eight feet high between the under side of the joices and the Surface of the Celler floor. And the foundation must go 12 Inches lower which will make the whole hight of the Celler Wall on which you lay the first floor 9 feet. This Wall shou'd be 19 Inches thick either of Stone or very hard Brick and the Partition Walls shoud be 14 inches thick. The first floor is designed 3 feet above the Surface of the Ground which will require the Wall about 2 feet or a little more raised above the said Surface. This part from the ground up to the top of the first floor shou'd be cased with hard Brick if the Celler Wall be of Stone, unless you go to the Expence of hewn Stone for this part which will be better. After the wall is worked up as high as the first floor to the full Demensions of the plan set off about 4 Inches for the finishing of the plinth or Water table which may be of Moulding Bricks. [Sketch included here]
The first Story is ten feet high from floor to Cieling. The outside Walls all round 14 Inches thick and the partitions nine Inches thick of Bricks. The second Story is designed the same thickness and to be Nine feet six Inches high. The Windows are 6 hights of Glass 10 by 8 Inches for the hight and 3 for the Width. There must be a grate of Iron to the inside of each Window which may be fixed in the following Manner. Suppose this to be the Jaums of a Window and Irons fixed ready to receive the grates when the Building is finished. [Sketch here] I woud have 2 eyes of Iron made like the rough Scratch above, which shou'd be made of Common flat bar Iron with a hole of an Inch diameter to receive a hook which will be fixed to the Grate, the other End split and turned up or down one Inch and built in the Brick work. These two eyes shou'd be fixed about eight Inches above the bottom of the Window and two more fixed about the same distance 99 from the top of the window, the Grate having four hooks to fit into those eyes May be set in and a hasp fixed to the Grate at top that will fall on a Staple drove into the lintel over the Window head fix on a padlock the whole will be safe. See this rough Scratch. [Sketch here]
Dimensions of the Plan
| feet | ||
| The Keepers Apartment | 22 | |
| feet In: | ||
| 6 Rooms on one side | 11. 9 | 70.6 |
| 2 End Walls | 14 | 2.4 |
| 6 Ditto | 9 | 4.6 |
| 2 Water Tables | 4 | .8 |
| Whole length of Building | 100. | |
| feet in: | ||
| 2 Rooms | 10. 9 each | 21.6 |
| 1 Passage | 6. 2 | 6.2 |
| 2 Walls | 14 thick | 2.4 |
| 2 Ditto | 9 do. | 1.6 |
| 2 Water Tables | 4 do | .8 |
| Whole Width of Building | 32.2 | |
| N. B. The middle part projects 3 feet | 6 | |
| 38.2 |
If there shoud be occasion for Fire to warm the common Rooms, there may be Stoves fixed in the Partition between two Rooms with the Mouth open to the Passage, by which means they make fires and the mad People cannot come at them. They shou'd be fixed about two foot above the floor for fear of the Patients falling against the Stoves. See to the left hand on the Plan the place of two Stoves.[This sketch was apparently not included in the minute book]
This Building will require about Two hundred thousand Bricks each Brick about 8 3/4 Long 2 3/8 Thick and 4 1/4 Broad about 13 of such Bricks with Mortar will make one foot Superficial of a Nine Inch Wall or 19 1/2 of such to a fourteen Inch Wall. The Bricklayers must order it so that the Chimneys come out in the Roof at Equal distance from the middle otherwise they will have a very ill Effect. This may be easily done.
About 40 Thousand feet of Scantling will be wanted Superficial, which we reckon at one Inch 12 such feet makes one foot Cubical Measure.
16 Thousand feet of plank for Doors and floors about 1 ½ Inch thick 2 Thousand feet of plank very good for Sashes &c.
1005 Thousand of Inch Boards for Cornice to the Eves and other finishing besides Boarding the Roof.
The above hints and a careful inspection of the plan may be sufficient to perform any part of the Building.
Philadelphia April 9, 1770 Robt. Smith
Court of Directors' Minutes, Eastern State Hospital, December 10, 1770 - July 23, 1801, pp. 13-15, Virginia State Library, Richmond.APPENDIX B
ARTICLES OF AGREEMENT BETWEEN BENJAMIN POWELL AND THE COURT OF DIRECTORS
Articles of Agreement indented made and concluded this the eighteenth day of January in the year-of our Lord one thousand seven hundred and seventy one Between Benjamin Powell of the City of Williamsburg carpenter of the one part and the Court of Directors of the Hospital for the Reception of Ideots Lunatics and persons of insane and disordered Minds of the other part Witnesseth that the said Benjamin Powell for and in consideration of the sum of Money herein after mentioned doth covenant and agree with the said Court of Directors that he will erect a large brick Building for an Hospital for the Reception of Ideots Lunatics and persons of insane and disordered Minds on the Lots lately purchased by the said Court of Directors of Thomas Walker agreable to the plan and explanation thereof hereto annexed The whole Wall of hard well burnt Bricks and laid with good Mortar the North front of the middle Building to have a neat Pediment the South East and West ends to be hipped to have a neat Mundelian Cornice round the whole the Roof to be covered with plank and good Cypress Shingles the Frame and Scantling to be of good Oak or poplar and of proper Sizes for such a Building the Floors to be laid with good pine Plank well seasoned one and a half Inch thick and free from Sap the outward Doors and those to the Middle Rooms to be panelled and the others strong batten Doors and the said Benjamin Powell doth agree to furnish all the materials for the said Building except the Grates and such other things as are usually imported from England and that he will finish and compleat the whole in a neat strong and workman like manner agreable to the plan and explanation thereof aforesaid within two years from the date hereof In Consideration whereof the said Court of Directors do agree to pay the said Benjamin Powell one thousand and seventy pounds in the following manner that is to say two hundred and fifty pounds part thereof in hand and the Residue at such Times and in such proportions as the said Court of Directors shall think fit to direct having regard to the progress of the Work.
In Witness whereof the parties to these presents have 102 hereunto set their Hands and affixed their Seals the day and Year before written.
Court of Directors' Minutes, Eastern State Hospital, December 10, 1770 - July 23, 1801, pp. 15-16, Virginia State Library, Richmond.Signed Sealed and Delivered
In the presence of Ben. Powell [seal]
Will Russell to B. P.
Henry TazewellSigned and seald. by W. Nelson [seal]
Wm. Nelson in presence of Geo. Nicholas
SELECTED READINGS
Many good secondary sources can be found on the history of hospitals and asylums in Europe and America. Two excellent works specifically on the Public Hospital in Williamsburg are Shomer Zwelling's Quest For A Cure (Williamsburg, 1985) and Norman Dain's Disordered Minds (Williamsburg, 1971). Another very good work on a specific American hospital is Nina Little's Early Years of the McLean Hospital (Boston, 1972). For general reading on both European and American hospitals there are a number of informative works: David Rothman's The Discovery of the Asylum (Boston, 1971); Leonard Eaton's New England Hospitals, 1790-1883; Gerald Grob's Mental Institutions in America (New York, 1973); William Parry-Jones' The Trade in Lunacy (London, 1972); Andrew Scull's Museums of Madness (London, 1979); Vieda Skultan's English Madness (London, 1979); and Nancy Tomes' A Generous Confidence: Thomas Story Kirkbride and the Art of Asylum-Keeping 1840-1883 (Cambridge, 1984).
The best material, however, is always contemporary. Writings on eighteenth-century hospitals in Europe include John Aikin's Thoughts on Hospitals (London, 1771) and John Howard's The State of Prisons (London, 1777) and An Account of the Principal Lazarettos in Europe (London, 1789). Howard, the legendary reformer of prisons, documents both the prevalence of 104 keeping the mentally ill in lazarettos and prisons and the despicable conditions of those places.
The early treatises on Moral Managment hospitals in Europe, primarily England and Scotland, are perhaps the most interesting: Andrew Duncan's Observations on the Structure of Hospitals for the Treatment of Lunatics as a Branch of Medical Police (Edinburgh, 1809); Observations on Hospitals for the Cure of Insanity, with essays by Robert Reid, Dr. Andrew Duncan, Jr., and Dr. Edward Fox (Edinburgh, 1809); Parliment's Report of Committee for Better Regulation of Madhouses (London, 1815); Philippe Pinel's Treatise on Insanity (1806); William Stark's Remarks on the Construction of Public Hospitals for the Cure of Mental Derangement (Glasgow, 1810); Samuel Tuke's Description of the Retreat (1813) and Practical Hints on the Construction and Economy of Pauper Lunatic Ayslums (1815); and Watson and Pritchett's Plans, Elevations, Sections and Description of the Pauper Lunatic Asylum, Lately Erected at Wakefield (York, 1819). Later European works on Moral Managment that were widely read in America were William Browne's What Asylums Were, Are and Ought to be (Edinburgh, 1837); John Conolly's The Construction and Government of Lunatic Asylums and Hospitals for the Insane (London, 1847) and Treatment of the Insane Without Mechanical Restraints (London, 1856); Sir Andrew Halliday's A General View of the Present State of Lunatics, and Lunatic Asylums in Great Britain and Ireland, and in Some Other Kingdoms (London, 1828); 105 and Maximilian Jacobi's On the Construction and Managment of Hospitals for the Insane (1841). Moral Managment works about American hospitals include John Bucknill's Notes on Asylums For the Insane in America (1876) and Thomas Kirkbride's On the Construction, Organization and General Arrangement of Hospitals for the Insane (1854).
There are, of course, many rich records and documents associated with the various mental institutions in America, not the least being those of Eastern State Hospital (at the hospital in Williamsburg and in the state archives in Richmond) and of the Galt Family (at the College of William and Mary).
Of particular architectural interest are three works: John Thompson and Grace Goldin's The Hospital: A Social and Architectural History (New Haven, 1975); Thomas Markus (ed.) Order in Space and Society (Edinburgh, 1982); and Anthony King (ed.) Buildings and Society (London, 1980).